BioMed Central
Page 1 of 5
(page number not for citation purposes)
Cough
Open Access
Case report
Achalasia: unusual cause of chronic cough in children
Nighat F Mehdi1, Miles M Weinberger2 and Mutasim N Abu-Hasan*2
Address: 1Pediatrics Pulmonary Section, University of Oklahoma, 940 NE 13th Street, Room 3B 3314, Oklahoma City, OK 73104, USA and
2Pediatric Allergy and Pulmonary Division, 2544 JCP, University of Iowa, 200 Hawkins Dr, Iowa City, IA 52242, USA
Email: Nighat F Mehdi - Nighat-Mehdi@ouhsc.edu; Miles M Weinberger - miles-weinberger@uiowa.edu; Mutasim N Abu-Hasan* - mutasim-
abu-hasan@uiowa.edu
* Corresponding author
Abstract
Achalasia is a rare motility disorder of the esophagus which results from lack of enervation of the
lower esophageal sphincter muscles and leads to dilatation of proximal esophagus. Patients with
achalasia presents typically with dysphagia, vomiting of undigested food and failure to thrive. Cough
can be present in achalasia patients due to aspiration of food or due to airway compression by the
dilated esophagus. We report two cases of achalasia presenting primarily with prolonged cough.
Diagnosis of achalasia in both cases was delayed due to this atypical presentation. This highlights
the importance of recognizing achalasia as a potential cause of chronic cough in order to avoid
delayed diagnosis and mismanagement.
Background
Achalasia is a disorder of esophageal motility which
occurs rarely in children [1]. Achalasia is caused by loss of
inhibitory enervation of lower esophageal sphincter and
is characterized by failure of the sphincter to relax. This
failure of relaxation causes poor emptying of the esopha-
gus and subsequent dilatation and abnormal contractility
of the proximal esophagus. The most commonly present-
ing symptoms of achalasia include dysphagia, chest pain,
vomiting, belching, regurgitation of undigested food and
failure to thrive. Cough can occur in achalasia primarily
due to aspiration of the undigested food particles or air-
way compression from dilated esophagus[2].
Due to its rare occurrence, achalasia is not commonly
thought of in evaluating children with chronic cough and
diagnosis can be consequently delayed. We report two
cases of achalasia in children presenting primarily with
chronic cough.
Case 1
A 9-your old girl presented for evaluation of 18 month
history of nocturnal cough and post-tussive emesis.
Cough occurred mainly at nighttime, occasionally trig-
gered by exercise and was almost always followed with
non-bilious vomiting of semi-digested food. Several
courses of antibiotics had been given with no improve-
ment in symptoms. Codeine containing cough suppres-
sants were only temporarily effective. There was no
response to albuterol inhaler, oral antihistamines and
nasal steroids. Besides cough and post-tussive emesis,
patient's parents also described less bothersome symp-
toms of nausea, gagging and epigastric pain. Past medical
history was remarkable for being diagnosed with pneu-
monia a year ago and with bronchiolitis in infancy.
On examination, she was above the 25th percentile for
weight and above the 75th percentile for height. Vital signs
were normal. Chest exam showed no signs of respiratory
Published: 24 July 2008
Cough 2008, 4:6 doi:10.1186/1745-9974-4-6
Received: 10 October 2007
Accepted: 24 July 2008
This article is available from: http://www.coughjournal.com/content/4/1/6
© 2008 Mehdi et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cough 2008, 4:6 http://www.coughjournal.com/content/4/1/6
Page 2 of 5
(page number not for citation purposes)
distress and was clear to auscultation. Initial evaluation
showed normal chest x-ray, normal lung spirometry, nor-
mal exercise challenge, and negative skin testing to com-
mon inhaled allergens.
Combined endoscopy and bronchoscopy were done
under conscious sedation. Endoscopy identified no
abnormality of the esophagus or stomach. Bronchoscopy,
on the other hand, showed oval shaped trachea at its mid
portion about 2.5 cm above the carina. The anterior and
posterior walls of the trachea approach each other, espe-
cially during vigorous coughing, and came to complete
contact on the right side creating a teardrop shaped
lumen. No abnormalities of the bronchi were observed.
Broncoalveolar lavage (BAL) fluid cell count contained
8% lymphocytes, 7% neutrophils, 10% eosinophils and
70% macrophages. BAL culture grew only mixed flora.
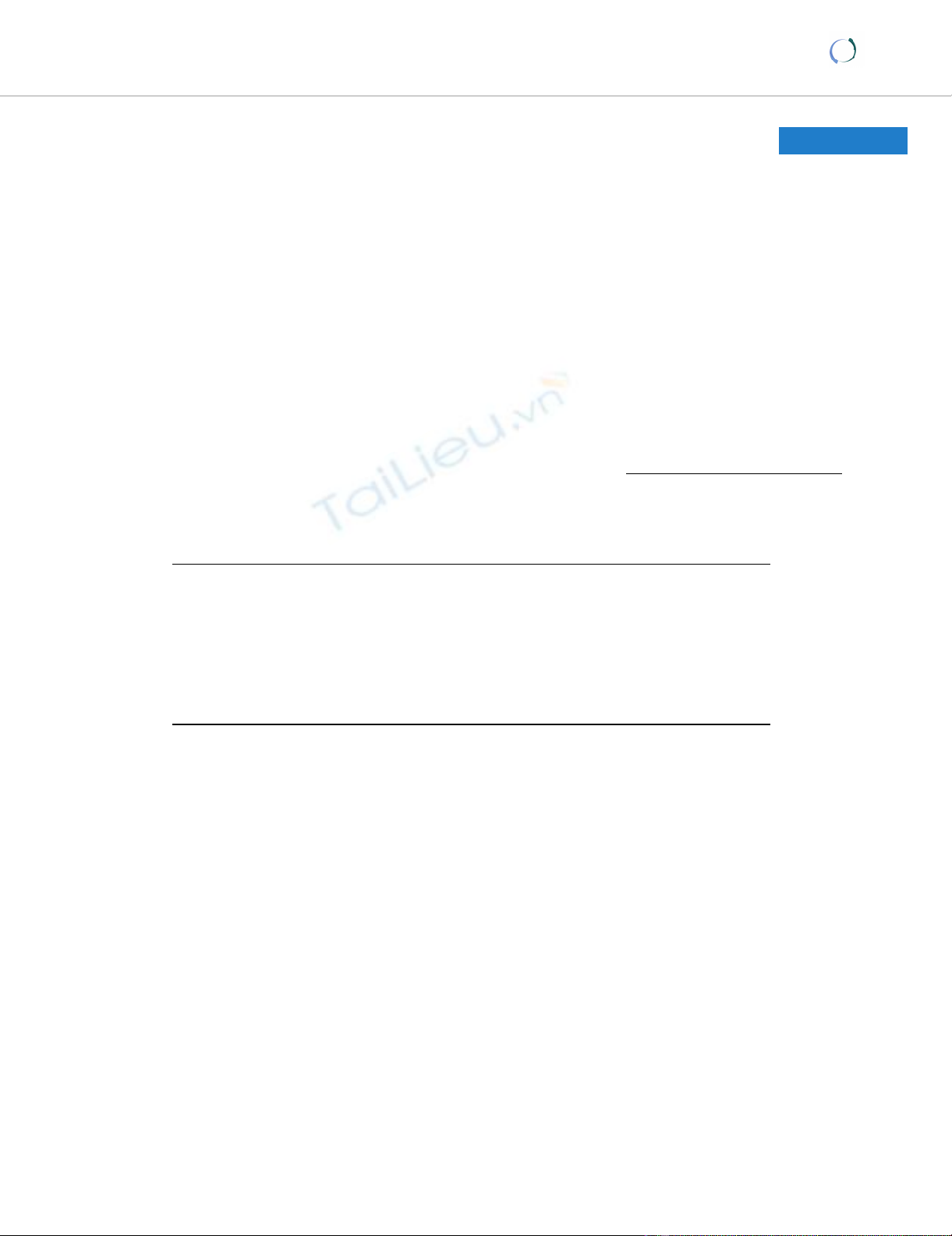
Because of the mid tracheal collapse observed during
bronchoscopy, a cine-CT with contrast was done to rule
out vascular ring with compression of the trachea. The CT
showed no abnormal vasculature but did show a large
dilated esophagus with air-fluid level from stagnant food
material (Figure 1). The trachea was compressed by the
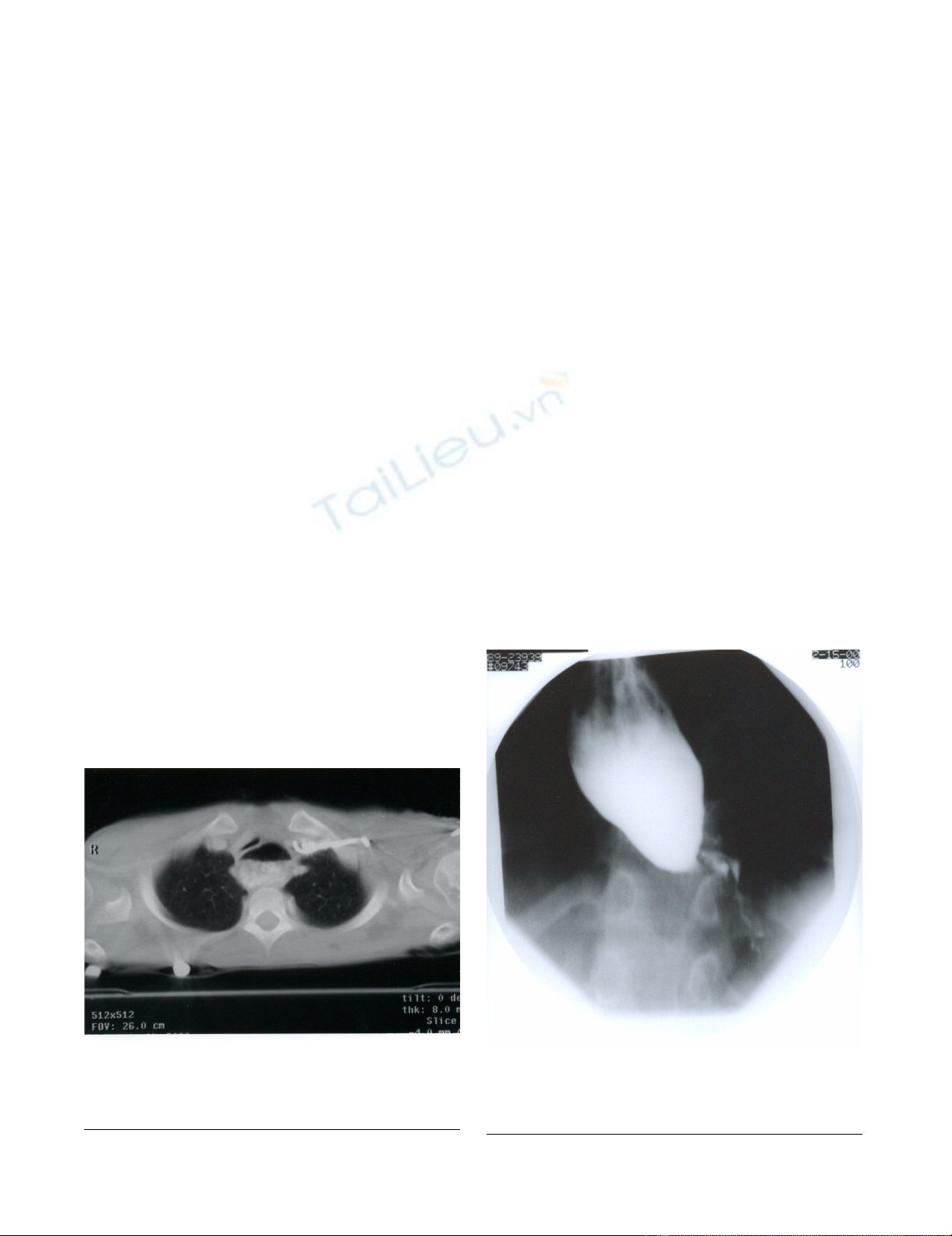
dilated esophagus and deviated towards the right. A Bar-
ium swallow study done later confirmed the diagnosis of
achalasia and demonstrated the presence of megaesopha-
gus with tapering and marked narrowing at the gastro-
esophageal junction causing functional obstruction with
significant delay of contrast passage into the stomach (fig-
ure 2). There were no primary peristalsis throughout most
of the esophagus and only non-peristaltic contractions
were seen. No aspiration was observed. Patient underwent
corrective surgical procedure after which the symptoms of
chronic cough disappeared.
Case 2
A 10-year old African-American female with Down syn-
drome was evaluated by our pulmonary service for history
of chronic daily cough and recurrent pneumonias for
eight and a half years duration. Cough was worse at night,
in supine position and during exertion. Cough also wors-
ened during viral respiratory tract infections. There was
history of frequent vomiting of undigested food but not
necessarily associated with the cough.
Patient was diagnosed with asthma exacerbations and
pneumonia and treated as such several times in her life-
time. She had history of transient clinical improvement
with antibiotics, bronchodilators and oral corticosteroids.
Daily inhaled corticosteroids failed to completely control
cough. Past medical history was significant for small ven-
tricular septal defect and chronic constipation.
On examination, she was between 75th and 90th percentile
for weight, and between 10th and 25th percentile for
height. Chest examination was unremarkable. Chest
roentgenograms showed predominantly patchy peribron-
chial air space consolidation with more involvement of
the right middle lobe. A Barium swallow study was first
Esophagogram showing severe dilatation of esophagus with smooth tapering at the gastroesophageal junctionFigure 2
Esophagogram showing severe dilatation of esopha-
gus with smooth tapering at the gastroesophageal
junction.
CT scan of chest showing dilatation of esophagus with air-fluid levelFigure 1
CT scan of chest showing dilatation of esophagus
with air-fluid level. Dilated esophagus is compressing the
trachea anteriorly.
Cough 2008, 4:6 http://www.coughjournal.com/content/4/1/6
Page 3 of 5
(page number not for citation purposes)
done at 5 years of age. There was no frank aspiration or
laryngeal penetration and the esophagogram revealed
normal anatomy of the esophagus with mildly delayed
hypopharyngeal contraction but no contrast retention.
Flexible bronchoscopy showed normal airway anatomy.
The BAL fluid contained 16% neutrophils, 35% lym-
phocytes, 35% macrophages with 14% percent epithelial
cells. Cultures grew only mixed flora. Lipid laden macro-
phages were present with Colombo index of 110 which is
consistent with aspiration[3].
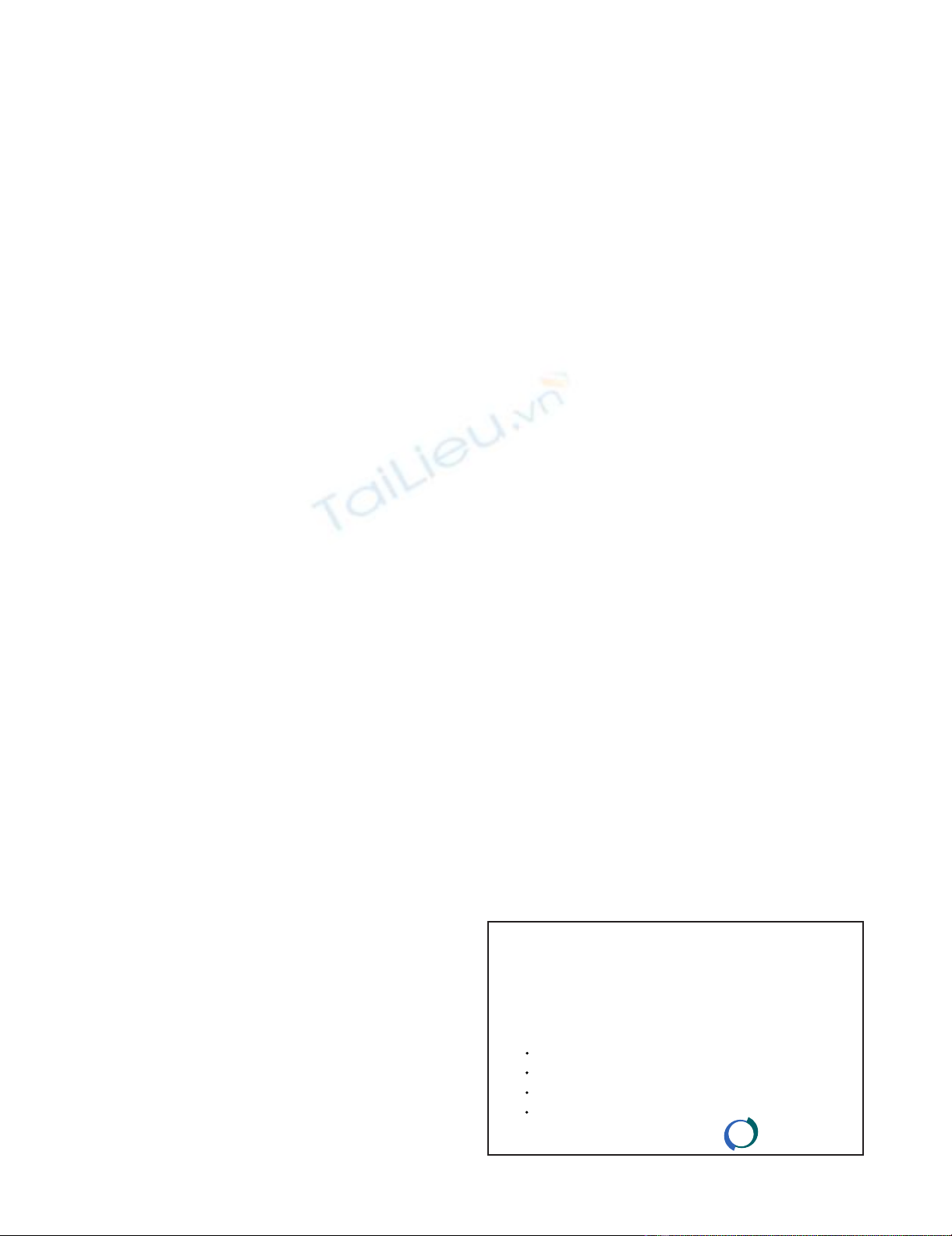
CT scan of the chest showed diffuse lung infiltrates that
seemed worse on right middle lobe and left lower lobe.
The esophagus was enlarged along its entire length but
with no obvious tracheal compression (figure 3). In view
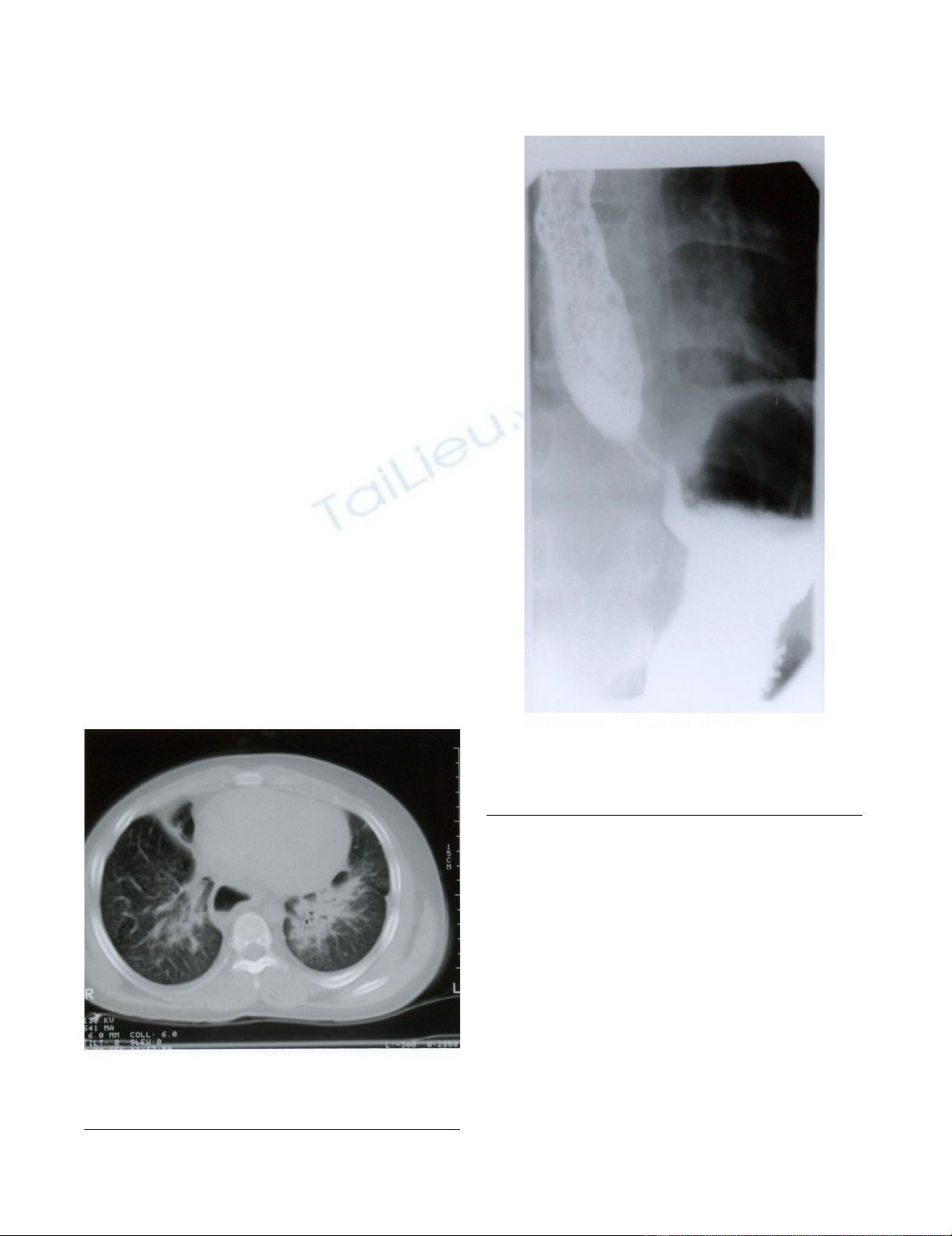
of the CT scan findings, a repeat Barium swallow study
was done which showed severe esophageal dysfunction
with multiple waves of tertiary contractions throughout a
markedly dilated thoracic esophagus. the distal esophagus
appeared tapered caudally with severe narrowing at the
gartroesophageal junction. Small food particles with air
bubbles were seen within the mid esophagus. Only small
amount of contrast passed to the stomach (figure 4).
Discussion
Achalasia is the most commonly recognized esophageal
motor disorder, first described 300 years ago by Sir Tho-
mas Willis[4,5]. It is an idiopathic esophageal motility
disorder, characterized by absence of normal peristalsis
and failure of relaxation of lower esophageal sphincter.
Achalasia occurs in the general population with a preva-
lence of eight per 100,000. It occurs mainly in adulthood,
with less than 5% of cases found before adolescence[1]. It
has been associated with other diseases such as Parkin-
son's disease, progressive cerebellar ataxia, familial gluco-
corticoid deficiency and Down syndrome[6,7].
Childhood achalasia is more common in boys[8]. Few
cases have been reported in infants [9]. Familial forms are
rare.
The most frequent symptoms of achalasia are dysphagia,
chest pain, regurgitation of food, and weight loss. Second-
ary pulmonary disease can occur due to regurgitation and
aspiration of retained esophageal contents. This can cause
symptoms of chronic cough, especially nocturnal cough,
choking, recurrent pulmonary infections, pneumonia,
Esophagogram showing diffuse dilatation of esophagus with tapering at gastroesophageal junctionFigure 4
Esophagogram showing diffuse dilatation of esopha-
gus with tapering at gastroesophageal junction.
Esophagus appears filled with food particles.
CT scan of chest showing bilateral lung opacification with septal thickening and esophageal dilatationFigure 3
CT scan of chest showing bilateral lung opacification
with septal thickening and esophageal dilatation.

Cough 2008, 4:6 http://www.coughjournal.com/content/4/1/6
Page 4 of 5
(page number not for citation purposes)
wheezing, atelectasis and rarely pulmonary empyema
[10]. Some patients may develop hoarseness of the voice
caused by direct pressure of distended esophagus on the
recurrent laryngeal nerve [11].
Tracheal obstruction due to compression from dilated
esophagus may occur in achalasia and can be the only
presentation [12]. This can be a serious and potentially
life threatening complication of achalasia [13,14].
Diagnosis of achalasia is suspected by the presence of
dilated esophagus with tapering of distal esophagus on
contrast esophagography (bird peak appearance). Esoph-
agography, however, suffers from low sensitivity as a diag-
nostic test [15]. CT scan of chest can also detect dilated
esophagus, esophageal wall thickening, and stagnant food
[16]. CT scan is particularity helpful in detecting associ-
ated comorbidities such as malignancies and lung infil-
trates [17]. The diagnostic value of chest CT for achalasia
compared to manometry has not been systematically
studied. Pressure manometry detects motility dysfunction
of the esophagus and failure of relaxation of the distal
esophageal sphincter and is considered the golden stand-
ard for diagnosis of achalsia. If biopsy of distal esophagus
is done, lack of myenteric plexus enervation can be dem-
onstrated.
In this report both cases presented with chronic nocturnal
cough as the main presenting symptoms of achalasia.
Other symptoms such as vomiting of undigested or semi
digested food was present but were not enough red-her-
ring to raise suspicion for diagnosis. Diagnosis of achala-
sia was finally reached after prolonged history of
symptoms and after several non-diagnostic evaluations
and several empirical therapies. Interestingly, diagnosis in
both cases was made by CT scan finding of dilated
esophagus and then confirmed by esophagography show-
ing the dilated, tapering and dysfunctional esophagus.
Even though, an esophagogram was done earlier in the
second case, the diagnosis of achalasia was not made on
that study. Meanwhile, patient continued to have cough
and recurrent aspiration pneumonia. The severely dilated
esophagus was seen years later on the CT scan and became
more obvious in the second esophagogram.
The second case had more severe complications from
aspiration than the first case despite similar age of presen-
tation. This could be due to poor airway clearance and the
non-specific immune compromise associated with tri-
somy 21. The presence of esinophilia in the brochoalveo-
lar lavage could not be clearly explained. It could possibly
reflect an associated atopic airway inflammation or
asthma.
The presence of trachea compression on the CT scan in the
first case suggests that tracheal compression was the
mechanism of chronic cough. On the other hand, the
presence of extensive pulmonary infiltrates on the chest
CT scan and the high lipid laden macrophage index in the
BAL fluid suggests that chronic aspiration was the mecha-
nism of chronic cough in the second case [[18,19],20].
In conclusion, both cases clearly demonstrate that achala-
sia could present primarily as chronic cough due to tra-
cheal compression from dilated esophagus and/or
chronic aspiration from regurgitated food. They also dem-
onstrate that failure to entertain the likelihood of achala-
sia as a cause of chronic cough could result in late
diagnoses and unwarranted morbidity.
Consent
The patients are lost to our follow-up, so obtaining con-
sent is not possible. Verbal consent was obtained by the
treating physicians and the coauthors (Dr. Mehdi and Dr.
Weinberger)
Authors' contributions
All authors conceived of the study, and participated in its
design and coordination. All authors read and approved
the final manuscript
References
1. Wong RK, Maydonovitch CL: Achalasia. In The esophagus Edited by:
Castell DO. Boston. Little Brown and Company; 1992:233-260.
2. Colombo JL, Hallberg TK: Recurrent aspiration in children:
lipid-laden alveolar macrophage quantitation. Pediatr Pulmonol
1987, 3(2):86-89.
3. Farr CM: Achalasia: new thoughts on an old disease. J Clin Gas-
troenterol 1992, 15(1):2-4.
4. Cash BD, Wong RK: Historical perspective of achalasia. Gas-
trointest Endosc Clin N Am 2001, 11(2):221-234.
5. Zarate N, Mearin F, Hidalgo A, Malagelada JR: Prospective evalua-
tion of esophageal motor dysfunction in Down's syndrome.
Am J Gastroenterol 2001, 96(6):1718-1724.
6. Nihoul-Fekete C, Bawab F, Lortat-Jacob S, Arhan P: Achalasia of
the esophagus in childhood. Surgical treatment in 35 cases,
with special reference to familial cases and glucocorticoid
deficiency association. Hepatogastroenterology 1991,
38(6):510-513.
7. Myers NA, Jolley SG, Taylor R: Achalasia of the cardia in chil-
dren: a worldwide survey. J Pediatr Surg 1994, 29(10):1375-1379.
8. Starinsky R, Berlovitz I, Mares AJ, Versano D, Pajewsky M, Modai D:
Infantile achalasia. Pediatr Radiol 1984, 14(2):113-115.
9. Akritidis N, Gousis C, Dimos G, Paparounas K: Fever, cough, and
bilateral lung infiltrates. Achalasia associated with aspiration
pneumonia. Chest 2003, 123(2):608-612.
10. Kugelman A, Berkowitz D, Best LA, Bentur L: Upper airway
obstruction as a presenting sign of achalasia in childhood.
Acta Paediatr 2000, 89(3):356-358.
11. Chapman S, Weller PH, Campbell CA, Buick RG: Tracheal com-
pression caused by achalasia. Pediatr Pulmonol 1989, 7(1):49-51.
12. Givan DC, Scott PH, Eigen H, Grosfeld JL, Clark JH: Achalasia and
tracheal obstruction in a child. Eur J Respir Dis 1985, 66(1):70-73.
13. Akhter J, Newcomb RW: Tracheal obstruction secondary to
esophageal achalasia. J Pediatr Gastroenterol Nutr 1988,
7(5):769-772.
14. El-Takli I, O'Brien P, Paterson WG: Clinical diagnosis of achalasia:
how reliable is the barium x-ray? Can J Gastroenterol 2006,
20(5):335-337.
Publish with BioMed Central and every
scientist can read your work free of charge
"BioMed Central will be the most significant development for
disseminating the results of biomedical research in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
Cough 2008, 4:6 http://www.coughjournal.com/content/4/1/6
Page 5 of 5
(page number not for citation purposes)
15. Rabushka LS, Fishman EK, Kuhlman JE: CT evaluation of achalasia.
J Comput Assist Tomogr 1991, 15(3):434-439.
16. Carter M, Deckmann RC, Smith RC, Burrell MI, Traube M: Differen-
tiation of achalasia from pseudoachalasia by computed tom-
ography. Am J Gastroenterol 1997, 92(4):624-628.
17. Smith Hammond C: "Cough and aspiration of food and liquids
due to oral pharyngeal Dysphagia". Lung 2008, 186(Suppl
1):S35-40.
18. Robinson GV, Kanji H, Davies RJ, Gleeson FV: Selective pulmo-
nary fat aspiration complicating oesophageal achalasia. Tho-
rax 59(2):180.
19. Akritidis N, Gousis C, Dimos G, Paparounas K: Fever, cough, and
bilateral lung infiltrates. Achalasia associated with aspiration
pneumonia. Chest 2003, 123(2):608-12.



![PET/CT trong ung thư phổi: Báo cáo [Năm]](https://cdn.tailieu.vn/images/document/thumbnail/2024/20240705/sanhobien01/135x160/8121720150427.jpg)






















%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)