BioMed Central
Page 1 of 4
(page number not for citation purposes)
Cough
Open Access
Case report
Gastroesophageal reflux-associated chronic cough in an adolescent
and the diagnostic implications: a case report
Makiko Jinnai1, Akio Niimi*1, Masaya Takemura2, Hisako Matsumoto1,
Yoshitaka Konda3 and Michiaki Mishima1
Address: 1Department of Respiratory Medicine, Kyoto University, Shogoin, Sakyo-ku, Kyoto, 606-8507, Japan, 2Department of Respiratory
Medicine, The Tazuke Kofukai Medical Research Institute Kitano Hospital, 2-4-20 Ohgimachi, Kita-ku, Osaka, Japan and 3Department of Internal
Medicine, Japan Baptist Hospital, 47 Yamanomoto-cho, Kitashirakawa, Sakyo-ku, Kyoto, 606-8273, Japan
Email: Makiko Jinnai - majin43@kuhp.kyoto-u.ac.jp; Akio Niimi* - niimi@kuhp.kyoto-u.ac.jp;
Masaya Takemura - masaya.takemura@charite.de; Hisako Matsumoto - hmatsumo@kuhp.kyoto-u.ac.jp;
Yoshitaka Konda - ykonda@msa.biglobe.ne.jp; Michiaki Mishima - mishima@kuhp.kyoto-u.ac.jp
* Corresponding author
Abstract
A 15-year-old girl was referred with a 2-year history of perennial non-productive cough, which had
been preceded by Mycoplasma pneumoniae pneumonia and subsequent asthma. Symptoms were
only partially responsive to anti-asthma treatment including an inhaled corticosteroid and a
leukotriene receptor antagonist. The patient's BMI was 27.8; she had gained over 10 kg in the
previous two years. Typical symptoms of gastroesophageal reflux disease were not evident except
for belch. Coughing worsened on eating and rising from bed. Although esophagography failed to
disclose reflux esophagitis, esophageal pH monitoring revealed significant acid reflux. Asthma was
considered well controlled. Treatment with the proton-pump inhibitor rabeprazole resulted in
disappearance of cough. Frequency Scale for the Symptoms of Gastroesophageal reflux disease
(FSSG) score, a questionnaire evaluating the symptoms of gastroesophageal reflux disease, was
initially high but normalized after treatment. Capsaicin cough sensitivity also diminished with
treatment.
Chronic cough due to gastroesophageal reflux disease has been considered rare in adolescents, but
this condition might be increasing in line with the recent trend in adults. Clinical features of
gastroesophageal reflux disease-associated cough typical for adult patients and a specific
questionnaire for evaluating gastroesophageal reflux disease validated in adults may also be useful
diagnostic clues in adolescents.
Background
Cough is the most common symptom for which patients
seek medical attention. In adults, cough variant asthma,
postnasal drip or rhinosinusitis, and gastroesophageal
reflux disease (GERD) are the most common causes of
chronic cough in Western countries[1]. In Japan, cough
variant asthma, sinobronchial syndrome, and atopic
cough have been considered the major causes of chronic
cough lasting for 8 weeks or longer[2], but the prevalence
of GERD is likely increasing [3-5], as has been reported in
Published: 15 July 2008
Cough 2008, 4:5 doi:10.1186/1745-9974-4-5
Received: 8 February 2008
Accepted: 15 July 2008
This article is available from: http://www.coughjournal.com/content/4/1/5
© 2008 Jinnai et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cough 2008, 4:5 http://www.coughjournal.com/content/4/1/5
Page 2 of 4
(page number not for citation purposes)
the USA[6]. There are far fewer studies of chronic cough
etiology in children than in adults, but GER is considered
rare, especially in adolescents [7-9].
We report a case of chronic cough due to GERD which pre-
sumably started at 13 years of age. Clinical features typical
in adult patients[10] and a specific questionnaire for eval-
uating GERD validated in adults[11] were useful in lead-
ing us to suspect GER-related cough before considering
esophagoscopy and esophageal pH monitoring.
Case Presentation
In February 2003, a 13-year-old girl was admitted to a
local hospital because of fever, cough and chest infiltrate
in X-ray. She was diagnosed as having Mycoplasma pneumo-
niae pneumonia from serology. Fever and chest infiltrate
resolved rapidly with antibiotic treatment, but cough and
wheezing persisted for several months. A diagnosis of
asthma was made, and treatment with inhaled
hydrofluoroalkane beclomethasone dipropionate 200 μg
bid and an leukotriene receptor antagonist pranlukast 225
mg bid was started. Although wheezing resolved with this
treatment, cough only partially improved and persisted.
In May 2005 she was again admitted to hospital due to an
exacerbation of coughing that prevented her attending
school, but investigations including laryngoscopy and
pulmonary function tests were normal. The patient was
referred and admitted to our department in June 2005
(Figure 1).
The patient was afebrile and in good general condition.
Her height and weight were 162 cm and 73 kg, respec-
tively, with a BMI of 27.8. Physical examination including
chest auscultation was normal, as were radiographs of the
chest and sinus. Methacholine airway hyperresponsive-
ness was positive, but spirometry results were normal as
indicated by an FVC of 3.8 L (120% of predicted value),
an FEV1 of 3.31 L (120%), and an FEV1/FVC of 87%. Bron-
chial reversibility was negative as demonstrated by pre-
and post-salbutamol FEV1 values of 3.31 L and 3.29 L,
respectively. Peak expiratory flow ranged from 420 to 440
L/min (variation < 5%), and eosinophil count in induced
sputum was normal (0.5%)[12]. Addition of inhaled sal-
meterol did not improve the patient's cough. These find-
ings indicated that asthma was well controlled, and
unlikely to be the cause of persistent cough. High resolu-
tion lung CT was unremarkable. Cough sensitivity to cap-
saicin was slightly heightened (C5, the lowest
concentration of capsaicin required to induce 5 coughs,
was 4.88 μM)[13].
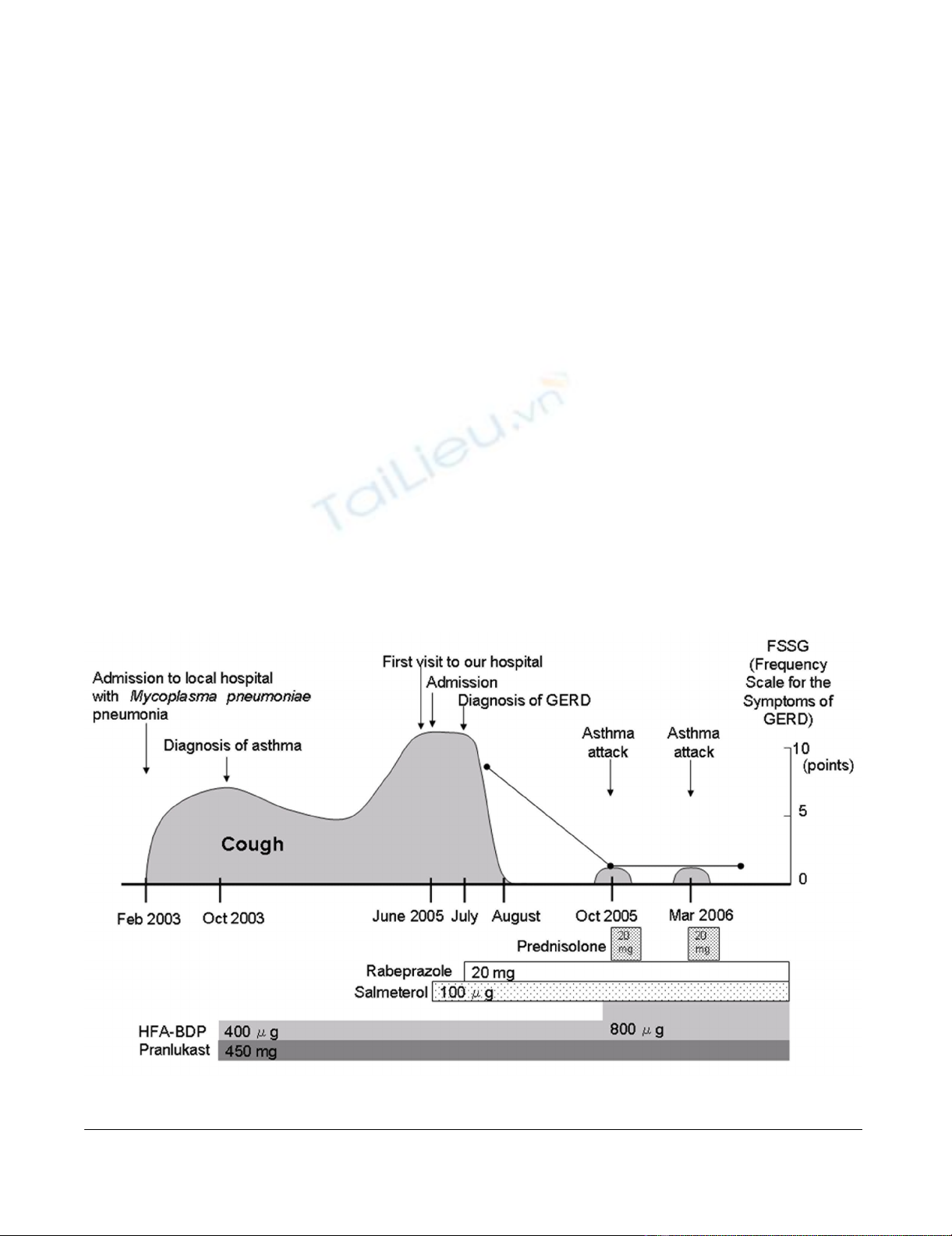
The patient's clinical courseFigure 1
The patient's clinical course.

Cough 2008, 4:5 http://www.coughjournal.com/content/4/1/5
Page 3 of 4
(page number not for citation purposes)
The patient lacked typical esophageal symptoms of GERD
such as heartburn or regurgitation, but complained of
belch. She was obese with a weight gain of over 10 kg in
the last two years. Cough was predominant in the daytime
and deteriorated on rising from bed and after eating. Fre-
quency Scale for the Symptoms of Gastroesophageal
reflux disease (FSSG) score, a questionnaire evaluating the
symptoms of GERD, was 9 points, which was higher than
the reference value (8 points)[11]. GER was accordingly
suspected as the cause of persistent cough. Esophagoscopy
failed to disclose reflux esophagitis, but 24-hour esopha-
geal pH monitoring revealed significant acid reflux: pH
was below 4.0 for 17% of the whole examination period;
this is 4 times higher than the reference value for children
(4%)[14] and that for adults (4.2%)[15]. Treatment with
rabeprazole, a proton-pump inhibitor, was started (20 mg
daily), and the patient's cough was markedly relieved,
eventually disappearing after 4 weeks of treatment. FSSG
score decreased to 2 points after 3 months, and after one
year C5 had also increased to 19.5 μM, indicating
improved sensitivity to capsaicin.
The patient remains on treatment for asthma and GERD
to date. In addition to continued use of rabeprazole, the
patient has lost 10 kg by following a reducing diet. She has
had several asthma exacerbations, but episodes have sub-
sided with short courses of oral prednisolone. Otherwise
coughing has been absent (Figure 1).
Discussion
Three prospective studies by Irwin et al. over a period of
17 years have shown that GERD has increased in impor-
tance as the cause of chronic cough in adults[6]: 10% (the
4th commonest cause) in 1981; 21% (3rd) in 1990[1];
and 36% (2nd) in 1998. Chronic cough due to GERD was
once considered rare in Japan[2], but among patients with
chronic cough at our clinic, GERD has increased as the
cause from 2% to around 10% over a decade [3-5] to
become the 3rd commonest cause[5].
Few studies have addressed the causes of chronic cough in
children, but available results suggest that GERD is rare as
a cause of isolated cough, especially in those aged 1 year
or older[7-9,16]. Marchant et al.[17] recently reported
that the prevalence of GERD in 108 children with cough
(median age 2.6 years; duration > 3 weeks) was 3.0% but
in none of the children was cough solely ascribed to
GERD. Holinger studied 38 children (aged 3 months to
15 years) with cough (> 4 weeks) but found only one with
GERD[7]. A later study by Holinger found GERD respon-
sible for cough (>4 weeks) in 11 out of 72 infants and
children[18]. In that study, although GERD was the most
common cause of cough among infants aged 18 months
or younger (9 of 32, 28%), it was the cause of cough in
only one of 22 children aged 6 to 16 years[18]. GERD
commonly occurs in infants[19] and becomes sympto-
matic during the first months of life, peaks by 4–5
months, and resolves by 12–24 months in most affected
babies[20,21]. This may explain the fact that high preva-
lence of GERD-associated cough is limited to very young
children[7,18]. The epidemiology of chronic cough in
Japanese children is poorly known, but the prevalence of
GERD may also have been low until recently. In a prelim-
inary investigation, coughing was attributed to GERD in
only 2 of 58 children (median age 5.2 years)[22]. How-
ever, the evidence in adults [3-6] leads us to suspect that
GERD might be increasing as a cause of chronic cough,
especially in older children or adolescents.
The golden standard for the diagnosis of GERD was 24-hr
esophageal pH monitoring formerly, but has recently
been taken place by multi-channel intraluminal imped-
ance-pH monitoring that can detect non-acid
reflux[23,24]. In any case, however, these examinations
are invasive and not widely available. As clinical clues to
the diagnosis of GERD, typical symptoms such as heart-
burn, regurgitation, and belch are important[9]. In a
recent study, the commonest symptoms of 47 adult
patients with chronic cough and objectively proven GER
included cough on phonation, cough on rising from bed,
cough on eating, and dysphonia[10]. Increased BMI has
been associated with symptoms of GERD, and even mod-
erate weight gain may cause or exacerbate symptoms of
reflux[25]. These features reported in adults were helpful
in raising the suspicion of GERD-related cough in our
patient. Such information has been scarce for children, as
gastroesophageal cough is considered rare in this age
group[26].
FSSG score is a simplified questionnaire for evaluating the
symptoms of GER, and it has been validated on the basis
of endoscopic evidence of reflux esophagitis in Japanese
adults[11]. When the cutoff score was set at 8 points, FSSG
had a sensitivity of 62%, a specificity of 59%, and an accu-
racy of 60%[11]. Moreover, its responsiveness to interven-
tion is high[11]. Our patient may be the first with GER-
associated chronic cough to demonstrate a high FSSG
score that responded well to treatment. The PPI was not
ceased to see if the cough recurred in our patient, but we
are confident that GERD was responsible for the patient's
longstanding cough that was quickly relieved by the PPI.
In our patient, cough was attributed to asthma before the
diagnosis of GERD was established. Chronic cough often
has dual causes, and GERD is an important consideration
because a self-perpetuating positive feedback cycle
between cough and GER has been demonstrated[27,28].
Cough from any cause may precipitate further reflux, lead-
ing to a vicious cycle of cough persistence[27,28]. When
cough improves only partially with conventional treat-
Publish with BioMed Central and every
scientist can read your work free of charge
"BioMed Central will be the most significant development for
disseminating the results of biomedical researc h in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
Cough 2008, 4:5 http://www.coughjournal.com/content/4/1/5
Page 4 of 4
(page number not for citation purposes)
ment of the primary diagnosis, coexistence of GERD
needs to be considered.
List of abbreviations
GERD: Gastroesophageal reflux; FSSG: Frequency scale for
symptoms of gastroesophageal reflux disease.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
MJ carried out the pulmonary function and methacholine
challenge tests and wrote the initial draft of the manu-
script. AN was responsible for disease diagnosis and man-
agement, revision of the manuscript, and supervision of
the study. MT carried out the capsaicin challenge test and
was also responsible for disease diagnosis and manage-
ment. HM participated in disease management. YK per-
formed the esophageal pH monitoring and interpreted
the results. MM supervised the study. All authors read and
approved the final manuscript.
Consent
Written informed consent was obtained from the patient
for publication of this case report and any accompanying
images. A copy of the written consent is available for
review by the Editor-in-Chief of this journal.
References
1. Irwin R, Curley F, French C: Chronic cough. The spectrum and
frequency of causes, key components of the diagnostic eval-
uation, and outcome of specific therapy. Am Rev Respir Dis
1990, 141:640-647.
2. Fujimura M, Abo M, Ogawa H, Nishi K, Kibe Y, Hirose T, Nakatsumi
Y, Iwasa K: Importance of atopic cough, cough variant asthma
and sinobronchial syndrome as causes of chronic cough in
the Hokuriku area of Japan. Respirology 2005, 10:201-207.
3. Niimi A: Geography and cough aetiology. Pulm Pharmacol Ther
2007, 20:383-387.
4. Matsumoto H, Niimi A, Takemura M, Ueda T, Yamaguchi M, Mat-
suoka H, Jinnai M, Chin K, Mishima M: Prevalence and clinical
manifestations of gastro-oesophageal reflux-associated
chronic cough in the Japanese population. Cough 2007, 3:1.
5. Niimi A, Ueda T, Chung K, Mishima M: Geographic difference in
chronic cough etiology: comparison between Japan and the
UK. Am J Respir Crit Care Med 2007, 175(abstract issue):A380
(abstract).
6. Irwin R: Chronic cough due to gastroesophageal reflux dis-
ease: ACCP evidence-based clinical practice guidelines. Chest
2006, 129:80S-94S.
7. Holinger L: Chronic cough in infants and children. Laryngoscope
1986, 96:316-322.
8. Chang A: Cough: are children really different to adults? Cough
2005, 1:7.
9. The Japanese respiratory society guidelines for management
of cough. Respirology 2006, 11(Suppl 4):S135-186.
10. Everett C, Morice A: Clinical history in gastroesophageal
cough. Respir Med 2007, 101:345-348.
11. Kusano M, Shimoyama Y, Sugimoto S, Kawamura O, Maeda M,
Minashi K, Kuribayashi S, Higuchi T, Zai H, Ino K, et al.: Develop-
ment and evaluation of FSSG: frequency scale for the symp-
toms of GERD. J Gastroenterol 2004, 39:888-891.
12. Gibson P, Fujimura M, Niimi A: Eosinophilic bronchitis: clinical
manifestations and implications for treatment. Thorax 2002,
57:178-182.
13. Niimi A, Matsumoto H, Ueda T, Takemura M, Suzuki K, Tanaka E,
Chin K, Mishima M, Amitani R: Impaired cough reflex in patients
with recurrent pneumonia. Thorax 2003, 58:152-153.
14. Ohhama Y, Suzuki N: Working group of Japanese society for
pediatric alimentary motility; Guidelines for pediatric 24-h
esophageal pH monitoring. Jpn J Pediatr Surg 1997:29.
15. Johnson L, Demeester T: Twenty-four-hour pH monitoring of
the distal esophagus. A quantitative measure of gastro-
esophageal reflux. Am J Gastroenterol 1974, 62:325-332.
16. Chang A, Widdicombe J: Cough throughout life: children, adults
and the senile. Pulm Pharmacol Ther 2007, 20:371-382.
17. Marchant J, Masters I, Taylor S, Cox N, Seymour G, Chang A: Eval-
uation and outcome of young children with chronic cough.
Chest 2006, 129:1132-1141.
18. Holinger L, Sanders A: Chronic cough in infants and children: an
update. Laryngoscope 1991, 101:596-605.
19. Hart J: Pediatric gastroesophageal reflux. Am Fam Physician
1996, 54:2463-2472.
20. Shepherd R, Wren J, Evans S, Lander M, Ong T: Gastroesophageal
reflux in children. Clinical profile, course and outcome with
active therapy in 126 cases. Clin Pediatr (Phila) 1987, 26:55-60.
21. Vandenplas Y, Lifshitz J, Orenstein S, Lifschitz C, Shepherd R,
Casaubón P, Muinos W, Fagundes-Neto U, Garcia Aranda J, Gentles
M, et al.: Nutritional management of regurgitation in infants.
J Am Coll Nutr 1998, 17:308-316.
22. Mochizuki H, Morikawa A: Nanchisei-gaisou-no- rinshou-to-
chiryohou. Asthma Frontier 2003, 2:66-75. (in Japnaese).
23. Vakil N, van Zanten S, Kahrilas P, Dent J, Jones R: The Montreal
definition and classification of gastroesophageal reflux dis-
ease: a global evidence-based consensus. Am J Gastroenterol
2006, 101:1900-1920. quiz 1943
24. Eastburn M, Katelaris P, Chang A: Defining the relationship
between gastroesophageal reflux and cough: probabilities,
possibilities and limitations. Cough 2007, 3:4.
25. Jacobson B, Somers S, Fuchs C, Kelly C, Camargo CJ: Body-mass
index and symptoms of gastroesophageal reflux in women.
N Engl J Med 2006, 354:2340-2348.
26. Marchant J, Masters I, Taylor S, Chang A: Utility of signs and symp-
toms of chronic cough in predicting specific cause in chil-
dren. Thorax 2006, 61:694-698.
27. Laukka M, Cameron A, Schei A: Gastroesophageal reflux and
chronic cough: which comes first? J Clin Gastroenterol 1994,
19:100-104.
28. Ing A: Cough and gastro-oesophageal reflux disease. Pulm Phar-
macol Ther 2004, 17:403-413.



![PET/CT trong ung thư phổi: Báo cáo [Năm]](https://cdn.tailieu.vn/images/document/thumbnail/2024/20240705/sanhobien01/135x160/8121720150427.jpg)






















%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)