Open Access
Available online http://ccforum.com/content/11/5/R98
Page 1 of 6
(page number not for citation purposes)
Vol 11 No 5
Research
Interference by new-generation mobile phones on critical care
medical equipment
Erik Jan van Lieshout1,2, Sabine N van der Veer3, Reinout Hensbroek4, Johanna C Korevaar5,
Margreeth B Vroom1 and Marcus J Schultz1,6
1Department of Intensive Care Medicine, Academic Medical Centre, University of Amsterdam, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands
2Mobile Intensive Care Unit, Academic Medical Centre, University of Amsterdam, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands
3Department of Medical Engineering, Academic Medical Centre, University of Amsterdam, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands
4Department of Prevention and Health, Netherlands Organisation for Applied Scientific Research, Zernikedreef 9, 2333 CK Leiden, The Netherlands
5Department of Clinical Epidemiology, Biostatistics and Bioinformatics, Academic Medical Centre, University of Amsterdam, Meibergdreef 9, 1105
AZ Amsterdam, The Netherlands
6Laboratory of Experimental Intensive Care and Anaesthesiology, Academic Medical Centre, University of Amsterdam, Meibergdreef 9, 1105 AZ
Amsterdam, The Netherlands
Corresponding author: Erik Jan van Lieshout, e.j.vanlieshout@amc.nl
Received: 18 Apr 2007 Revisions requested: 24 May 2007 Revisions received: 12 Jun 2007 Accepted: 6 Sep 2007 Published: 6 Sep 2007
Critical Care 2007, 11:R98 (doi:10.1186/cc6115)
This article is online at: http://ccforum.com/content/11/5/R98
© 2007 van Lieshout et al.; licensee BioMed Central Ltd.
This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction The aim of the study was to assess and classify
incidents of electromagnetic interference (EMI) by second-
generation and third-generation mobile phones on critical care
medical equipment.
Methods EMI was assessed with two General Packet Radio
Service (GPRS) signals (900 MHz, 2 W, two different time-slot
occupations) and one Universal Mobile Telecommunications
System (UMTS) signal (1,947.2 MHz, 0.2 W), corresponding to
maximal transmit performance of mobile phones in daily
practice, generated under controlled conditions in the proximity
of 61 medical devices. Incidents of EMI were classified in
accordance with an adjusted critical care event scale.
Results A total of 61 medical devices in 17 categories (27
different manufacturers) were tested and demonstrated 48
incidents in 26 devices (43%); 16 (33%) were classified as
hazardous, 20 (42%) as significant and 12 (25%) as light. The
GPRS-1 signal induced the most EMI incidents (41%), the
GRPS-2 signal induced fewer (25%) and the UMTS signal
induced the least (13%; P < 0.001). The median distance
between antenna and medical device for EMI incidents was 3
cm (range 0.1 to 500 cm). One hazardous incident occurred
beyond 100 cm (in a ventilator with GRPS-1 signal at 300 cm).
Conclusion Critical care equipment is vulnerable to EMI by
new-generation wireless telecommunication technologies with
median distances of about 3 cm. The policy to keep mobile
phones '1 meter' from the critical care bedside in combination
with easily accessed areas of unrestricted use still seems
warranted.
Introduction
Electromagnetic interference (EMI) with medical equipment by
second-generation mobile phones has been reported exten-
sively and seems clinically relevant to about 10% of medical
devices [1-7]. The growth in use and the decrease in size of
mobile phones intensifies the discussion on present hospital
restrictions on the use of mobile phones in patient areas,
which is violated by healthcare workers themselves to improve
patient care by better communication [8]. Critical incidents
caused by mobile phones are probably rare but are potentially
lethal and are most probably not recognized as such [9,10].
First-generation mobile phones are mainly used for voice,
whereas new generations of telecommunication systems ena-
ble us to have wireless internet access to send and receive
data even at the patient's bedside [11]. Data transmission may
be of more concern in the context of EMI. However, these new
systems entered the market with limited proof of their safety in
CDMA = code-division multiple access; EMI = electromagnetic interference; GPRS = General Packet Radio Service; GSM = Global System for
Mobile Communications; UMTS = Universal Mobile Telecommunications System.

Critical Care Vol 11 No 5 van Lieshout et al.
Page 2 of 6
(page number not for citation purposes)
the critical care environment [12]. Unfortunately, studies on
EMI-induced incidents are characterized by a technical
description of incidents only, whereas classification of their
clinical relevance is needed to update evidence-based poli-
cies on the use of modern mobile phones [3,13].
The aim of the present study was to assess and classify inci-
dents of EMI by second-generation and third-generation tele-
communication signals on 61 critical care devices.
Methods
Medical equipment
In all, 61 different medical devices (27 different manufactur-
ers) in 17 categories were allocated for EMI tests (Table 1).
The details of the devices are summarized in Additional file 1.
All devices were tested in accordance with an international
test protocol during full operation and in different modes; a
simulator (namely an electrocardiogram simulator, an artificial
lung and a syringe filled with saline) was connected if relevant
[14]. The tests were performed on devices in use for patient
care by two different hospitals (Academic Medical Center,
Amsterdam, The Netherlands, and Kennemer Gasthuis, Haar-
lem, The Netherlands) to maximize the number of devices; sim-
ilar test conditions were used in each location.
Signals
The General Packet Radio Service (GPRS) signals had time-
slot durations of 1,113 μs and a repetition frequency of 217
Hz (GRPS-1) or 556.5 μs at 27.1 Hz (GPRS-2), both with a
0.2 MHz channel bandwidth and a carrier frequency of 900
MHz. This GPRS technology, based on time-division multiple-
access technology and available for data transfer in Europe,
the United States, Australia and parts of Asia, was chosen for
its forthcoming use for data transmission [11]. GPRS is con-
sidered a 2.5-generation wireless telephony system.
The Universal Mobile Telecommunications System (UMTS)
signal had a bandwidth of 5 MHz and a carrier frequency of
1,947.2 MHz. This wideband code-division multiple-access
frequency-division duplex technology is considered a third-
generation wireless telephony system. A signal generator (HP/
Agilent E4433B/ESG-D Digital RF 250 kHz to 4 GHz), pro-
vided with a Global System for Mobile Communications
(GSM)/W-CDMA module, was used in combination with
external control equipment (a laptop and an additional pulse
generator) for timing purposes. The signals were amplified and
their power level was controlled at 2 W for GRPS in active
time slots and at 0.2 W for UMTS. These power levels corre-
spond to maximal transmit performance of mobile phones in
daily practice and were chosen to mimic a worst-case but real-
istic scenario to maximize the chance of detecting EMI-related
incidents.
The signals were radiated towards the medical apparatus
through an electrically balanced handheld antenna without
reflecting obstacles nearby. Special attention was paid to
poorly shielded locations in device housings (such as connec-
tors, sensors, and seams in the housing). The initial distance
between antenna and device was 500 cm from the device
housing and was decreased to 0 cm or until any incident
occurred [14]. In the event of any interference the test was
repeated three times to assess reproducibility.
Classification of incidents
Incidents observed during the normal operation of each device
were documented in detail. Two board-certified and experi-
enced intensivists classified by consensus of opinions the
severity of the observed incidents in accordance with an
adjusted scale of critical care adverse events [15]. The scale
ranges from light (influence on monitoring without a significant
level of attention needed, for example a disturbed display)
through significant (influence on monitoring with a significant
level of attention needed, causing substantial distraction from
patient care, for example an incorrect alarm or inaccurate mon-
itoring of blood pressure) to hazardous (direct physical influ-
ence on the patient by an unintended change in equipment
function, for example total stopping of ventilator or syringe
pump).
Statistical analysis
Median, maximum and minimum are given if no normal distribu-
tion was established. Distances are expressed in centimetres.
The distance between the antenna and device was set at 0.1
cm if an incident occurred when the antenna was held against
the housing of the device. Percentages of critical care devices
disturbed by second-generation and third-generation telecom-
munication signals (GPRS-1, GPRS-2 and UMTS) were com-
pared by using Cochran's Q test. The difference between
median distances between antenna and device at which inci-
dents occurred were analysed with the Friedman test. A linear-
by-linear χ2 test was performed to test for a trend in the fre-
quency of incidents in relation to the year of purchase of the
device.
Results
EMI by GPRS or UMTS signals on critical care medical equip-
ment was demonstrated in 26 of the 61 device tests (43%)
(Table 1). A total of 48 incidents were identified and classified
as 16 (33%) hazardous, 20 (42%) significant and 12 (25%)
light.
The GPRS-1 signal induced the highest number of incidents
of EMI: 41% (25 of 61), followed by GRPS-2 (25%; 15 of 61)
and UMTS (13%; 8 of 61; P < 0.001). The same was true of
the hazardous incidents: GPRS-1 20% (12 of 61), GPRS-2
5% (3 of 61) and UMTS 2% (1 of 61; P < 0.001). The medical
devices and descriptions of all incidents are listed in Addi-
tional file 1.
Available online http://ccforum.com/content/11/5/R98
Page 3 of 6
(page number not for citation purposes)
Hazardous incidents occurred in devices for therapy only due
to the definitions of the adjusted critical adverse events scale.
In mechanical ventilators, nine hazardous incidents (in seven
ventilators out of nine tested; median distance 3 cm, range 0.1
to 300) varied from 'total switch-off and restart' to changes in
set ventilation rate. In syringe pumps, two hazardous incidents
(in two pumps out of seven tested; distances 0.1 and 2 cm)
demonstrated a complete stop without an acoustic alarm or
with an incorrect alarm. One hazardous incident in a renal
replacement device (out of five machines tested; distance 15
cm) showed a stop after an incorrect air detector alarm. One
external pacemaker (out of three tested; distance 3 cm) dem-
onstrated a hazardous incident, with incorrect inhibition of the
pacemaker.
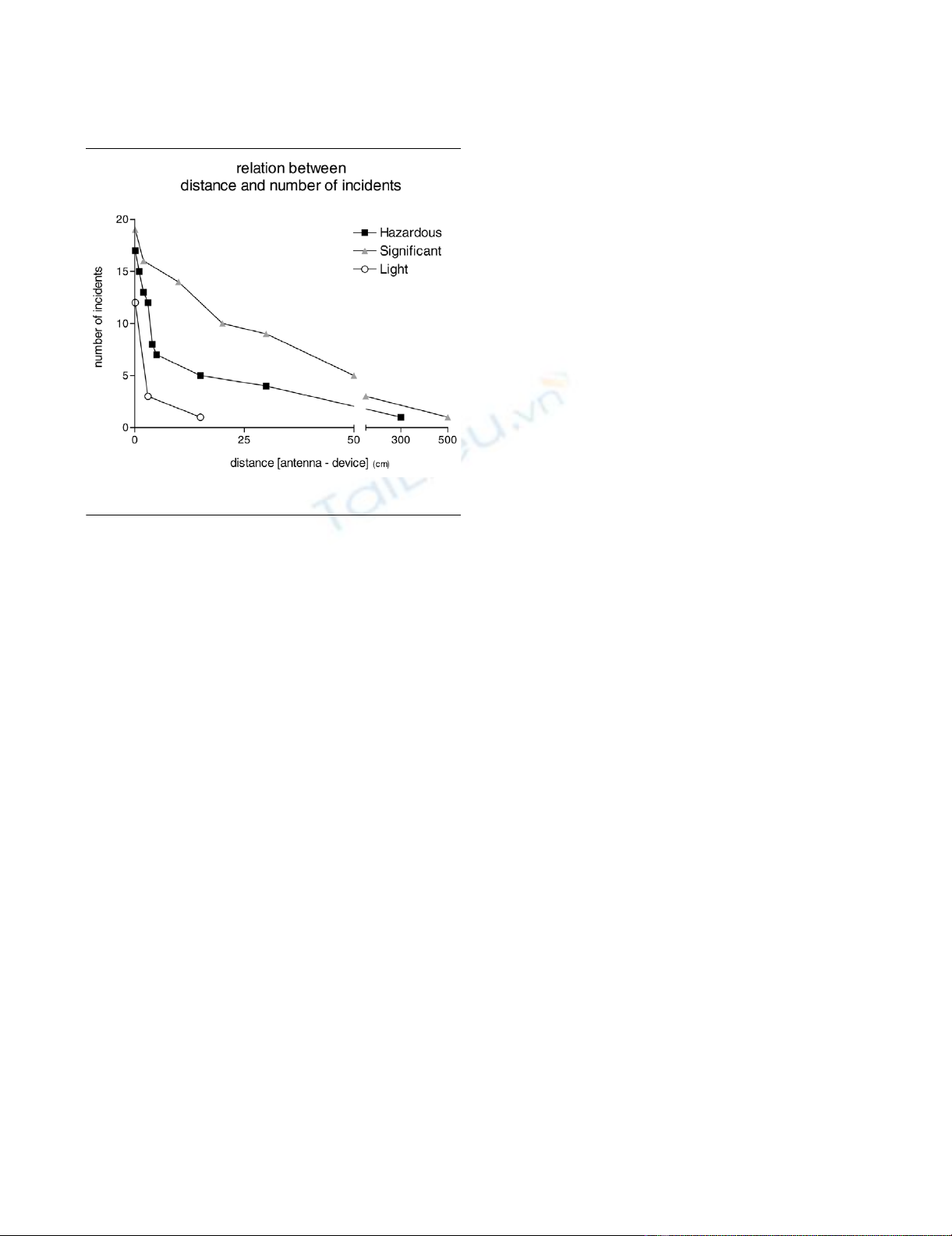
The median distance between antenna and device at which all
type of incident occurred was 3 cm, range (0.1 to 500 cm).
The relation between distance and number of hazardous, light
and significant incidents is depicted in Figure 1.
Incidents occurred at greater distance with the GPRS-1 signal
(median 5 cm) than with the GPRS-2 (median 3 cm) or UMTS
(median 1 cm) signal, although the differences were not statis-
tically significant (P = 0.12).
Hazardous incidents occurred at a median distance of 3.5 cm
(range 0.1 to 300 cm). Beyond 100 cm one hazardous inci-
dent at 300 cm in a ventilator with the GRPS-1 signal and two
significant incidents occurred at 150 cm in a 12-lead electro-
cardiogram device with GPRS 1, GPRS-2 and UMTS signals
(see Additional file 1).
Table 1
Categories of medical devices, interference distances and type of incidents per signal
Type of device or incident Number of devices Distancea (cm) Type of incident per signalb
Tested Influenced GPRS-1 GPRS-2 UMTS
Intensive care unit ventilator 9 7 1.5 [0.1–300] 6H, 1L 2H, 1S, 1L 1H, 2S, 1L
Critical care monitor 13 7 3 [0.1–500] 4S, 3L 2S, 4L
Syringe pump 7 3 5 [0.1–50] 2H, 1S S S
Volumetric infusion pump 4 1 30 S S S
Intra-aortic balloon pump 2 1 0.1 L
Haemofiltration/dialysis 5 1 15 H
External pacemaker 4 1 3 H
Defibrillator 3 1 0.1 L
12-lead EKG 1 1 150 S S S
Fluid warmer 2 1 6 S S
Enteral feeding pump 2 1 30 H H
Air humidifier 1 1 5 H
EKG telemetry 1 0
Forced-air warming unit 3 0
Mobile suction unit 1 0
Critical care bed 2 0
Continuous-airflow mattress 1 0
Type of incidentb
Hazardous 3.5 [0.1–300]
Significant 25 [0.1–500]
Light 0.1 [0.1–3]
Total 61 26 (43%) 3 [0.1–500] 25 (41%) 15 (25%) 8 (13%)
GPRS, General Packet Radio Service; UMTS, Universal Mobile Telecommunications System; EKG, electrocardiogram. aResults are shown as
median [range]. bHazardous (H) is defined as a direct physical influence on patient by unintended change in equipment function; significant (S) is
defined as an influence on monitoring with a significant level of attention needed, causing substantial distraction from patient care; light (L) is
defined as an influence on monitoring without a significant level of attention needed.
Critical Care Vol 11 No 5 van Lieshout et al.
Page 4 of 6
(page number not for citation purposes)
No relation could be demonstrated between the year of pur-
chase of medical devices and the number of incidents (P =
0.67).
Discussion
The present study demonstrates two new findings in the field
of interference by mobile phones on medical equipment.
First, the 2.5-generation mobile communication network
GPRS is able to induce a higher rate of EMI incidents than is
known for the first-generation network GSM at comparable
distances [1,3,7]. Second, the median distance at which EMI
incidents caused by new-generation cellular phones take
place (3 cm) falls within the '1 meter rule' proposed as a safe
distance in patient areas, although the range demonstrated in
this study is considerable (0.1 to 500 cm) [1,5,11,16].
Studies on EMI by first-generation mobile phones have been
based on the GSM network used in Europe, the United States,
Australia and part of Asia, or on code-division multiple access
(CDMA), which is used mostly in the United States [2,3].
Meanwhile GPRS and UMTS networks are used for their
advanced properties to transmit video and data wirelessly at a
higher speed as well as regular voice telephony [12].
Our finding of EMI induced by UMTS with hazardous incidents
contrasts with what was demonstrated recently in the only
study so far on UMTS by Wallin and colleagues [12]. No criti-
cal UMTS incidents with 76 medical devices were reported
besides interference noise on loudspeakers of two ultrasonic
Doppler devices. Their only critical incident with GPRS was
the total stopping of one infusion pump (out of 12 tested) at a
distance of 50 cm. Neither GPRS nor UMTS demonstrated
any interference on four intensive care ventilators tested.
Three of those ventilators were also tested in our study, and in
contrast with those studied by Wallin and colleagues they
showed significant and hazardous GRPS incidents and one
light UMTS incident. There are two possible explanations for
these differences. First, Wallin and colleagues used a different
GPRS signal with a frequency of 1,800 MHz and an output
power of 1 W, as opposed to 900 MHz and 2 W used in the
present study. The lower carrier-wave frequency of the GPRS
signal and the corresponding 2 W in our study was chosen for
its availability in many continents. GPRS is used worldwide on
different frequency bands (900 and 1,800 MHz) in different
continents and therefore many 'tri-band or quad-band' mobile
phones are sold for their worldwide operation [3,13]. Second,
the studies differed in their selection from medical equipment
available worldwide. Our results apply to the tested devices
only as specified, including the year of purchase, and conse-
quently are a limitation of the present study.
Another limitation of this study is the test conditions. The only
method for obtaining reproducible results in testing EMI by
mobile phones is a standard signal generator to control output
power as used in the study by Wallin and colleagues and in
our own [3,12]. The use of commercially available mobile
phones in ringing mode will generate irreproducible results at
different locations because mobile phones (GSM, GPRS and
UMTS) regulate their output power depending on the nearest
cell base station for the telecom provider [4,17]. If such a sta-
tion is nearby, a mobile phone constantly minimizes its
required output power, in GPRS to as low as 5 to 10% (50 to
100 mW), to increase its battery lifespan. In our study the out-
put power was controlled and set at the maximum level to
mimic a worst-case but realistic scenario. In healthcare facili-
ties the coverage of telecommunication networks could be
poor because of its structures and could consequently induce
mobile phones to transmit at maximum power, which increases
the risk of EMI [1,12]. Therefore, as a result of our worst-case
scenario it is not to be expected that in daily practice critical
EMI incidents with GPRS or UMTS would be more frequent
than reported in our study.
Health care applications of new wireless telecommunication
technologies are reaching the bedside (namely intelligent
pager systems with smart phones, personal digital assistants
with internet access, and telemonitoring interhospital intensive
care transport) with potential clinical benefits [2,8]. However,
critical care equipment, with closed loop systems to eliminate
human resources and errors, demands permanent technology
assessment to ensure its continued performance including
electromagnetic compatibility with other devices [2].
The international standard on electromagnetic compatibility by
the International Electrotechnical Commission in its present
form is insufficient to safeguard medical equipment completely
from EMI by GSM mobile phones, and our results show that
the same holds true for GPRS and UMTS signals [11,18]. The
Figure 1
Relation between distance and number of incidentsRelation between distance and number of incidents.
Available online http://ccforum.com/content/11/5/R98
Page 5 of 6
(page number not for citation purposes)
present industrial standard lacks stipulations for eliminating
EMI in medical equipment. Manufacturers are allowed to com-
ply with the standard by reporting only the distance at which
EMI occurs. Reasons why even new medical devices still dem-
onstrate EMI caused by mobile phones would be speculative;
examples are complex medical industrial design, rapidly
changing telecommunications signals, and costs. This leads
one to suspect that the undesirable situation of EMI in the crit-
ical care environment will not be eradicated soon.
This study adds to the objective evidence that restrictive use
in the critical care environment is sensible without overstress-
ing negligible risks [11,19].
Conclusion
The '1 meter rule', specifying the minimum distance to keep a
mobile phone from medical equipment or the bedside as pro-
posed in the past, seems safe, although the rule does not
exclude EMI by new-generation mobile phones entirely.
Restrictive policies should be facilitated by offering numerous
areas that are easily accessed throughout the healthcare facil-
ity where the use of mobile phones is clearly permitted.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
EJvL designed the study, performed the measurements,
assisted in the statistical analyses and drafted the manuscript.
SNvdV designed the study, helped in performing the measure-
ments and interpreting the results and participated in drafting
the manuscript. RH designed the study, performed the meas-
urements and participated in drafting the manuscript. JCK per-
formed the statistical analysis and participated in drafting the
manuscript. MBV and MJS participated in the study design, in
interpreting the results and in drafting the manuscript. All
authors read and approved the final manuscript.
Additional files
Acknowledgements
The authors thank the Department of Medical Engineering, Academic
Medical Center, Amsterdam, the Kennemer Gasthuis Haarlem, Dave
Dongelmans MD, and Royal KPN N.V., The Hague, for their logistical
and technical assistance and expertise. RH received an unrestricted
research grant ('MICU Connected') from Royal KPN N.V. for the present
study.
References
1. Mobile Communications Interference [http:www.mhra.gov.uk/
home/idcplg?IdcServ ice=SS_GET_PAGE&nodeId=261]
2. International Organization for Standardization (ISO): Health Infor-
matics – Use of Mobile Wireless Communication and Computing
Technology in Healthcare Facilities Geneva: ISO; 2005. [Report
no. ISO/TR 21730:2005.]
3. Lawrentschuk N, Bolton DM: Mobile phone interference with
medical equipment and its clinical relevance: a systematic
review. Med J Aust 2004, 181:145-149.
4. Tri JL, Severson RP, Hyberger LK, Hayes DL: Use of cellular tel-
ephones in the hospital environment. Mayo Clin Proc 2007,
82:282-285.
5. Shaw CI, Kacmarek RM, Hampton RL, Riggi V, El Masry A, Cooper
JB, Hurford WE: Cellular phone interference with the operation
of mechanical ventilators. Crit Care Med 2004, 32:928-931.
6. Barbaro V, Bartolini P, Benassi M, Di Nallo AM, Reali L, Valsecchi
S: Electromagnetic interference by GSM cellular phones and
UHF radios with intensive-care and operating-room
ventilators. Biomed Instrum Technol 2000, 34:361-369.
7. Irnich WE, Tobisch R: Mobile phones in hospitals. Biomed
Instrum Technol 1999, 33:28-34.
8. Soto RG, Chu LF, Goldman JM, Rampil IJ, Ruskin KJ: Communi-
cation in critical care environments: mobile telephones
improve patient care. Anesth Analg 2006, 102:535-541.
9. Hahn IH, Schnadower D, Dakin RJ, Nelson LS: Cellular phone
interference as a cause of acute epinephrine poisoning. Ann
Emerg Med 2005, 46:298-299.
10. Anonymous: Wireless communication devices and electromag-
netic interference. ECRI's updated recommendations. Health
Devices 2001, 30:403-409.
11. Lapinsky SE, Easty AC: Electromagnetic interference in critical
care. J Crit Care 2006, 21:267-270.
12. Wallin MK, Marve T, Hakansson PK: Modern wireless telecom-
munication technologies and their electromagnetic compati-
bility with life-supporting equipment. Anesth Analg 2005,
101:1393-1400.
13. Ettelt S, Nolte E, McKee M, Haugen OA, Karlberg I, Klazinga N,
Ricciardi W, Teperi J: Evidence-based policy? The use of
mobile phones in hospital. J Public Health (Oxf) 2006,
28:299-303.
14. Institute of Electrical and Electronics Engineers: American
National Standard Recommended Practice for On-site ad hoc
Test Method for Estimating Radiated Electromagnetic Immunity of
Medical Devices to Specific Radio-frequency Transmitters
(Standard C63.18) Piscataway, NJ: IEEE; 1997.
15. Kivlahan C, Sangster W, Nelson K, Buddenbaum J, Lobenstein K:
Developing a comprehensive electronic adverse event report-
Key messages
• Incidents of EMI caused by second-generation and
third-generation mobile phones occurred in 43% of 61
critical care medical devices, of which 33% were classi-
fied as hazardous.
• The hazardous incidents varied from a total switch-off
and restart of a mechanical ventilator, through complete
stops without alarms in syringe pumps, to incorrect
pulsing by an external pacemaker.
• The median distance of all incidents was 3 cm, with a
considerable range up to 500 cm.
• The policy to keep mobile phones '1 meter' from the
critical care bedside in combination with easily
accessed areas of unrestricted use still seems
warranted.
The following Additional files are available online:
Additional file 1
An Excel file containing a list of medical devices and
descriptions of all incidents.
See http://www.biomedcentral.com/content/
supplementary/cc6115-S1.xls



![PET/CT trong ung thư phổi: Báo cáo [Năm]](https://cdn.tailieu.vn/images/document/thumbnail/2024/20240705/sanhobien01/135x160/8121720150427.jpg)






















%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)