by
Dr TRẦN NGỌC ÁNH
Hà Nội Medical University

Objectives
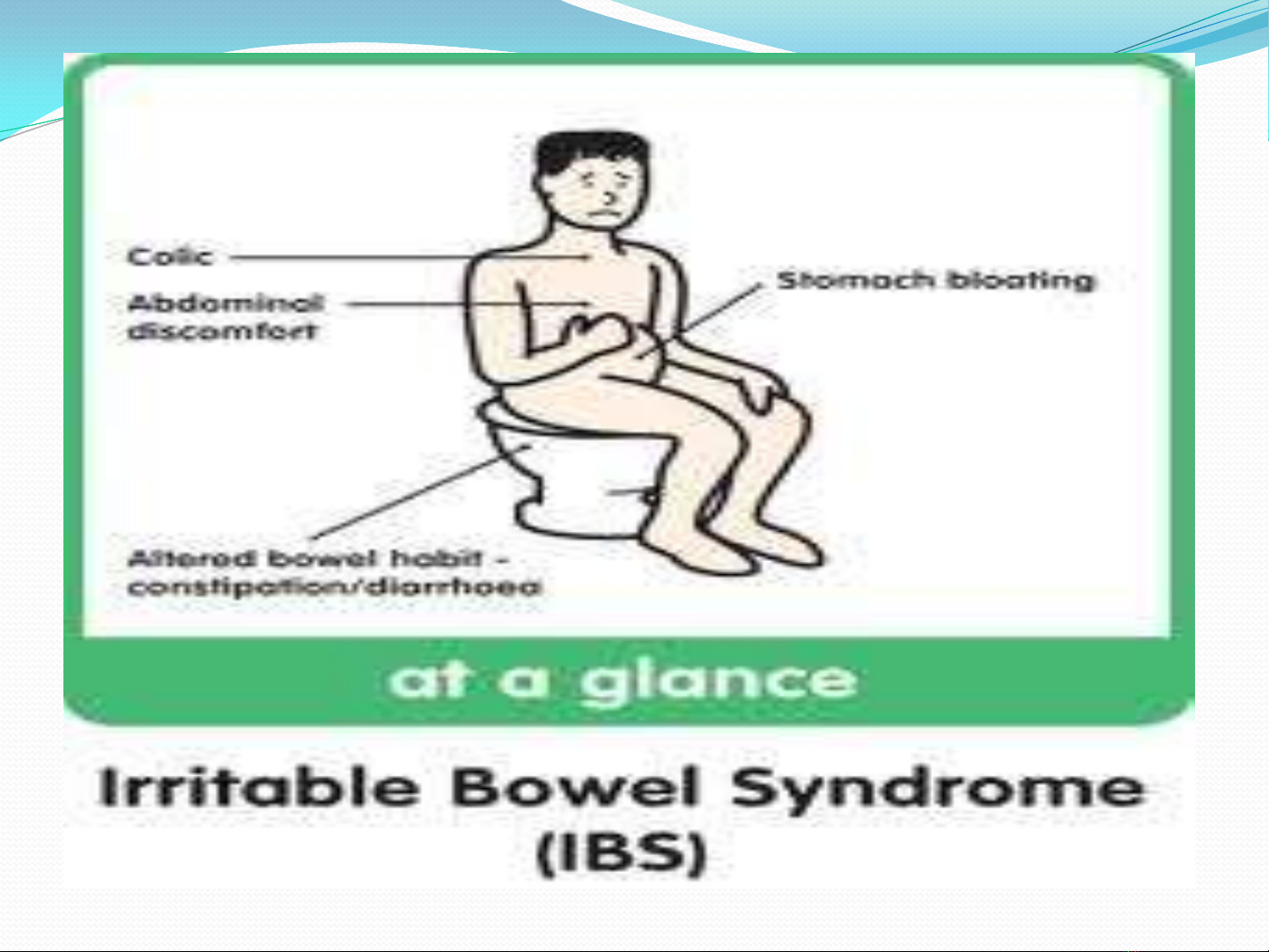
1.Recognize the typical
clinical presentation for
IBS
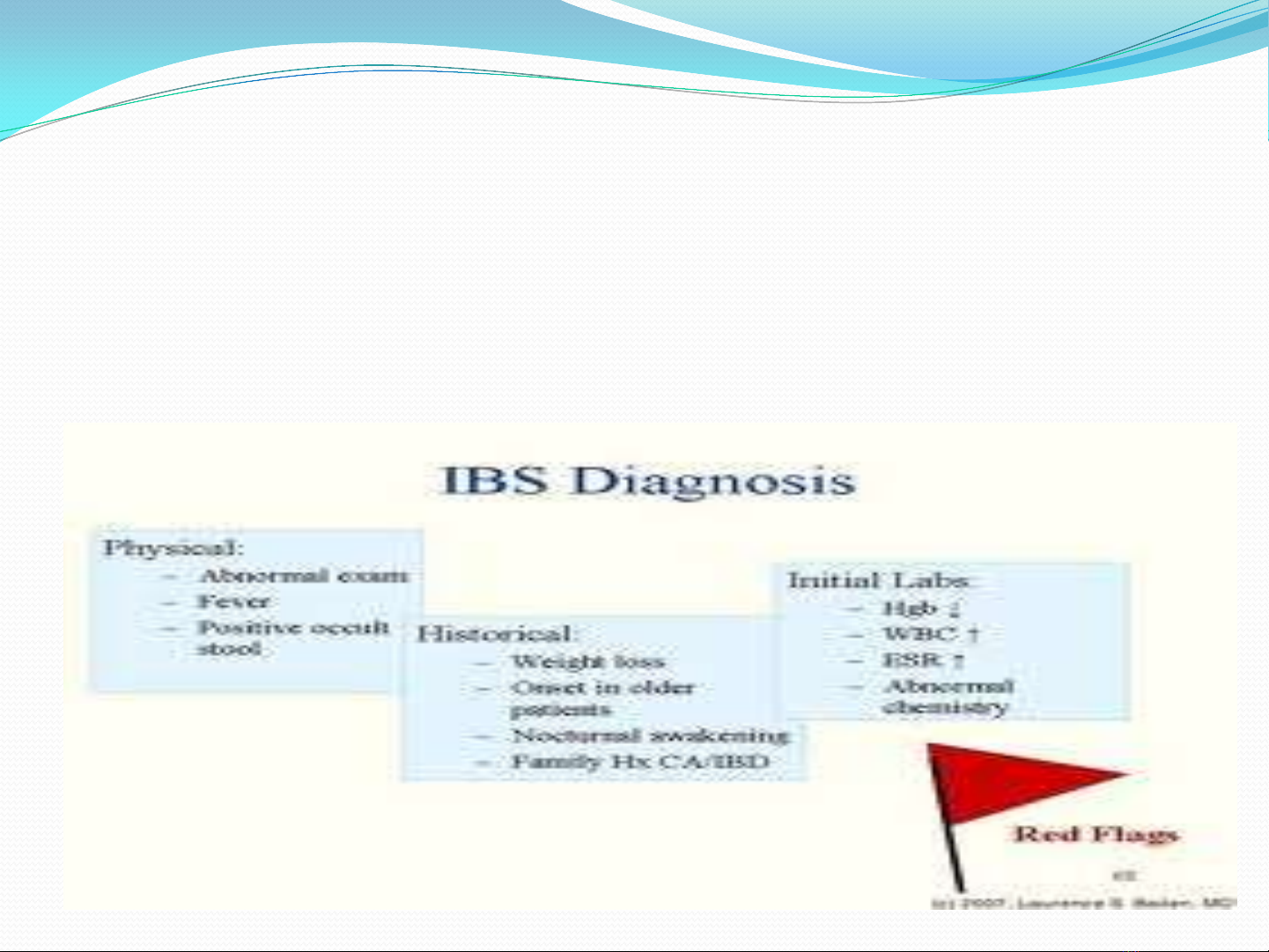
2.Describe an appropriate
diagnostic plan and ROME
III
3.Prescribe an appropriate
therapeutic regimens
IBS- Dr Trần Ngọc Ánh
GENERAL CONSIDERATIONS
IBS- a functional bowel disorder : abdominal pain,
discomfort, altered bowel habits, absence of detectable
structural abnormalities
IBS-other functional disordes: fibromyalgia, headech,
backache, genitourinary symptoms
IBS- Dr Trần Ngọc Ánh
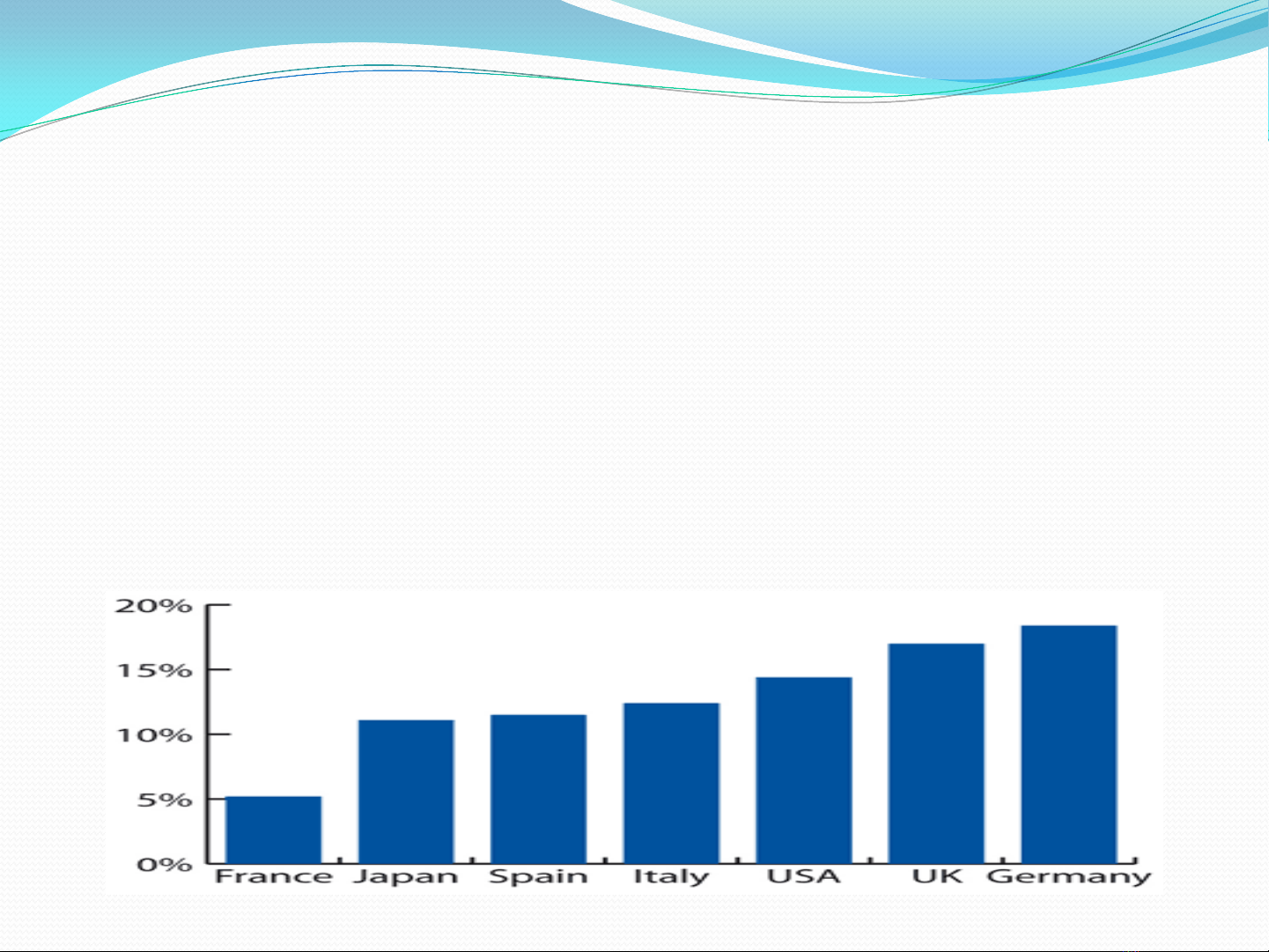
GENERAL CONSIDERATIONS
Diagnosis: Clinical presentation
10-20% adult, adolescents: symptoms of IBS
W/M:2-3; 80% Severe in women
IBS- Dr Trần Ngọc Ánh
IBS- Dr Trần Ngọc Ánh


![Điện Tâm Đồ: Bài giảng lớp kỹ năng đọc [chuẩn nhất]](https://cdn.tailieu.vn/images/document/thumbnail/2026/20260204/hoaphuong0906/135x160/63751770260074.jpg)

![Bài giảng xét nghiệm cơ bản trong thận học [mới nhất]](https://cdn.tailieu.vn/images/document/thumbnail/2026/20260123/lionelmessi01/135x160/38501769159065.jpg)








![Cẩm nang Huyết học [Chuẩn nhất]](https://cdn.tailieu.vn/images/document/thumbnail/2026/20260513/baobinh_011/135x160/6151778671287.jpg)



![Tài liệu lâm sàng Nhi khoa 2 [chuẩn nhất]](https://cdn.tailieu.vn/images/document/thumbnail/2026/20260508/baobinh_011/135x160/7771778235480.jpg)



![Tài liệu lâm sàng Nhi khoa 3: [Mô tả chi tiết hơn về nội dung tài liệu, ví dụ: Hướng dẫn chẩn đoán và điều trị bệnh ở trẻ em]](https://cdn.tailieu.vn/images/document/thumbnail/2026/20260508/baobinh_011/135x160/3591778237813.jpg)

![Tài liệu lâm sàng Nhi khoa 1: [Mô tả chi tiết, ví dụ: Hướng dẫn chẩn đoán và điều trị bệnh]](https://cdn.tailieu.vn/images/document/thumbnail/2026/20260508/baobinh_011/135x160/3691778238301.jpg)

