Open Access
Available online http://ccforum.com/content/11/6/R131
Page 1 of 5
(page number not for citation purposes)
Vol 11 No 6
Research
Induction of procalcitonin in liver transplant patients treated with
anti-thymocyte globulin
Roman Zazula1, Miroslav Prucha2, Tomas Tyll1 and Eva Kieslichova3
1Department of Anesthesiology and Intensive Care, Charles University in Prague, the First Faculty of Medicine and Thomayer's Faculty Hospital,
Videnska 800, 140 59 Prague, Czech Republic
2Department of Clinical Biochemistry, Hematology and Immunology, Hospital Na Homolce, Roentgenova 2, 150 30 Prague, Czech Republic
3Department of Anesthesiology and Intensive Care, Institute for Experimental and Clinical Medicine, Videnska 1958/9, 140 21 Prague, Czech
Republic
Corresponding author: Roman Zazula, roman.zazula@ftn.cz
Received: 1 Mar 2007 Revisions requested: 3 Apr 2007 Revisions received: 30 Aug 2007 Accepted: 18 Dec 2007 Published: 18 Dec 2007
Critical Care 2007, 11:R131 (doi:10.1186/cc6202)
This article is online at: http://ccforum.com/content/11/6/R131
© 2007 Zazula et al.; licensee BioMed Central Ltd.
This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction The aim of this study was to compare the early
postoperative kinetics of procalcitonin (PCT) and C-reactive
protein (CRP) serum levels in patients undergoing orthotopic
liver transplantation (OLTx) with different immunosuppressive
regimens.
Methods PCT and CRP serum concentrations were measured
in a group of 28 OLTx recipients before induction of anesthesia,
at 4 and 8 hours following graft reperfusion, and daily until
postoperative day 4. The same parameters were determined in
12 patients undergoing liver resection without conjunctive
immunosuppressive therapy. Summary data are expressed as
medians and ranges. Two-tailed nonparametric tests were
performed and considered significant at p values of less than
0.05.
Results The highest serum levels of PCT (median 3.0 ng/mL,
minimum 1.4 ng/mL, maximum 13.9 ng/mL) were found in
patients after OLTx without ATG therapy, on postoperative day
1. In patients with ATG administration, PCT levels were highly
increased on postoperative day 1 (median 53.0 ng/mL,
minimum 7.9 ng/mL, maximum 249.1 ng/mL). Thereafter, PCT
values continuously decreased independently of further ATG
administration in both groups of patients. No evidence of
infection was present in either group. In 12 patients undergoing
liver resection, peak serum PCT levels did not exceed 3.6 ng/
mL. CRP serum levels in a group of patients with and without
ATG therapy increased significantly on postoperative day 1,
followed by a decrease. The highest levels of CRP were found
in patients after liver resection on postoperative day 2 and
decreased thereafter.
Conclusion ATG administration to patients with OLTx is
associated with an increase in serum PCT levels, with peak
values on postoperative day 1, and this was in the absence of
any evidence of infection. The results of this study indicate that
ATG immunosuppressive therapy is a stimulus for the synthesis
of PCT.
Introduction
At the beginning of the '90s, it was discovered that elevated
levels of serum procalcitonin (PCT) were closely related to the
infectious etiology of systemic inflammatory response. Its role
as a marker of infectious inflammation was reported repeat-
edly, and today PCT is assessed as a sensitive and specific
marker of severe bacterial inflammation [1,2].
The last meta-analysis established that PCT is a more sensitive
and specific parameter for the evidence of systemic bacterial
infection than C-reactive protein (CRP) [2]. An increased PCT
level over the course of the first 24 hours is an independent
predictor of all-cause mortality in a 90-day follow-up period [3].
In patients undergoing organ transplantations, markers allow-
ing the differentiation between infectious complications and
rejection are of major clinical importance. Elevated PCT levels
have been detected in patients following organ transplantation
in a number of studies [4-6]. Mild PCT elevation can be a
marker of surgical trauma. In some studies, PCT was evaluated
ATG = anti-thymocyte globulin (polyclonal antibodies against human T cells); CRP = C-reactive protein; OKT3 = monoclonal antibody that specifically
reacts with the T cell receptor-CD3 complex on the surface of circulating human T cells; OLTx = orthotopic liver transplantation; PCT = procalcitonin.

Critical Care Vol 11 No 6 Zazula et al.
Page 2 of 5
(page number not for citation purposes)
for its sensitivity in distinguishing between acute rejection and
infection [4,7]. Highly elevated PCT levels were described in
patients having undergone immunosuppressive therapy. All
patients were post-liver or post-kidney transplantation and
were without the presence of systemic bacterial infection
[6,8,9].
The aims of the present study were (a) to investigate serum
levels of PCT and CRP in the perioperative and postoperative
periods in patients undergoing orthotopic liver transplantation
(OLTx) and receiving different perioperative inductive immuno-
suppressive therapy, (b) to address the possible molecular
relationship between the liver transplantation with conjunctive
immunotherapy and PCT production, and (c) toevaluate our
results in patients undergoing liver resection without immuno-
suppressive therapy.
Materials and methods
PCT and CRP levels were investigated in two groups of
patients undergoing OLTx with different regimens of the immu-
nosuppressive therapy and in one group of patients undergo-
ing liver resection as a surgical control. In the first group of
patients (n = 21), polyclonal antibodies against T lymphocytes
were administered together with the anti-thymocyte globulin
(ATG) (9 mg/kg) (Fresenius, Fresenius Biotech GmbH,
Gräfelfing, Germany) and methylprednisolone 250 mg during
the anhepatic phase. Afterward, patients received a combina-
tion of ATG (3 mg/kg up to postoperative day 3), cyclosporin
A (7.5 mg/kg per day), and methylprednisolone. In the second
group, 7 patients perioperatively received methylprednisolone
250 mg only. Subsequent therapy involved methylpred-
nisolone and tacrolimus (0.1 mg/kg per day FK 506, tac-
rolimus [Fujimycin] immunosuppressive drug, macrolide
antibiotic). The serum levels of PCT and CRP were measured
before the induction of anesthesia, in the fourth and eighth
hours after graft reperfusion, and continued daily to the fourth
day after surgery.
The third group involved 12 patients undergoing liver resec-
tion. No infectious complications were observed during the
early postoperative period (7 days). PCT and CRP levels were
measured before the induction of anesthesia, immediately
after the surgery, and then daily up to the fourth day after
surgery.
Infection was defined as a clinical or microbiological infection.
During the first 5 days, cultivation of urine and sputum as well
as chest x-ray were carried out on a routine basis. If the body
temperature exceeded 38°C, blood cultures were performed.
The study was approved by the local ethics committee. All bio-
logical material was sampled upon informed consent.
Blood samples
Procalcitonin and C-reactive protein measurements
Blood samples were collected as a routine test in accordance
with the ethical guidelines of the hospital. All blood samples
were stored at 4°C and were analyzed within 48 hours. PCT
analyses were performed using an immunoluminometric assay
(Lumitest-PCT; BRAHMS Aktiengesellschaft, Hennigsdorf,
Germany) Analyses of CRP were performed using a fully auto-
mated turbidimetric assay.
Statistical analysis
Summary data are expressed as median and range (minimum
and maximum). Two-tailed tests were performed and consid-
ered significant at p values of less than 0.05. The Friedman
nonparametric test was used to evaluate the time changes,
and the Kruskal-Wallis analysis of variance was used to evalu-
ate differences between groups.
Results
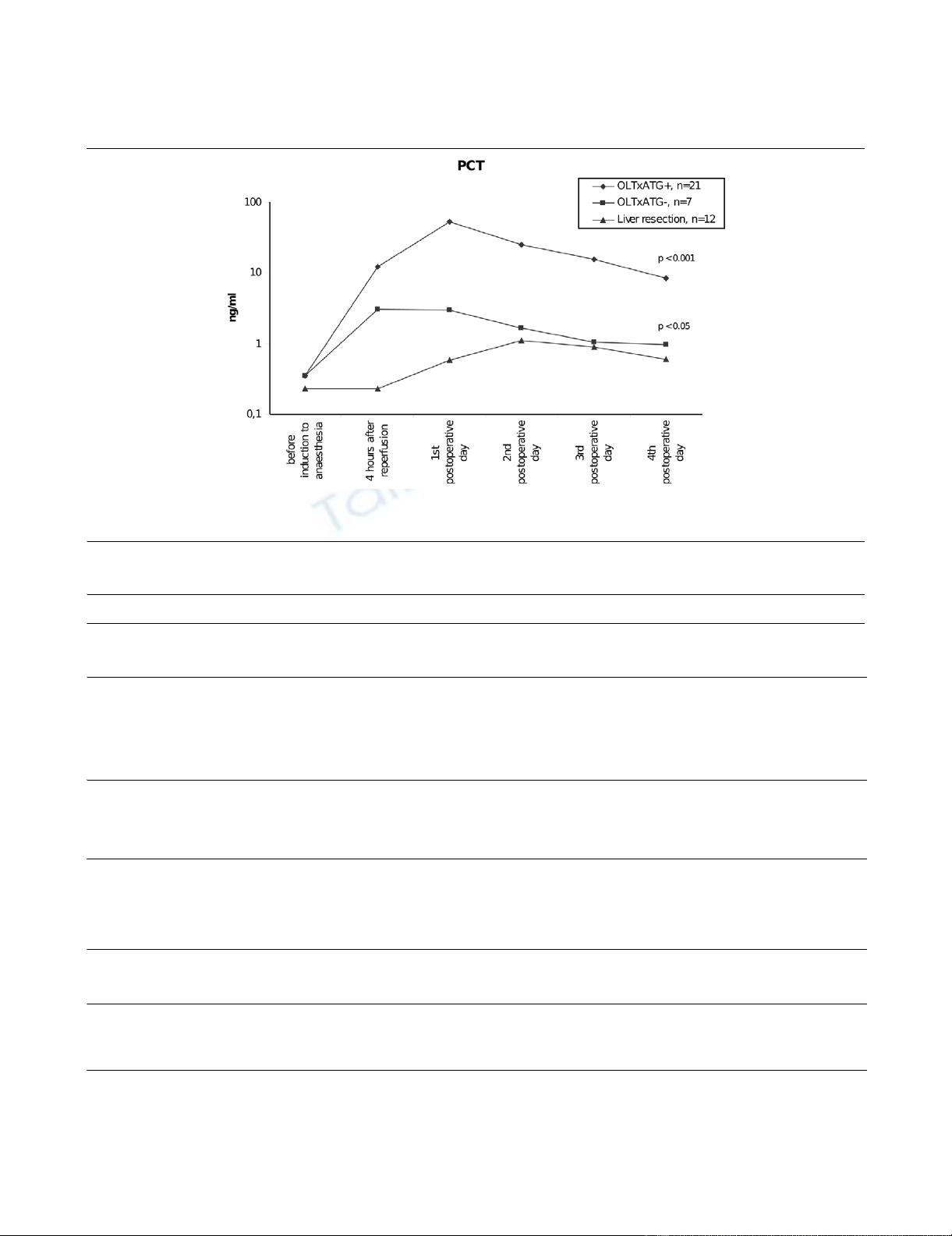
PCT levels were significantly higher in liver transplantation
patients with ATG therapy compared with patients without
ATG therapy, with a significant difference being detectable 4
hours after the graft reperfusion (p < 0.001). PCT levels were
significantly higher in both groups of patients undergoing liver
transplant and receiving immunosuppressive therapy in com-
parison with patients with liver resection alone (p < 0.05) (Fig-
ure 1).
In patients with ATG therapy, the median PCT level 4 hours
after reperfusion of the liver graft was 12.2 ng/mL (minimum
1.4 ng/mL, maximum 49.7 ng/mL), and the maximum levels
were detected on the first postoperative day (median 53 ng/
mL, minimum 7.9 ng/mL, maximum 249.1 ng/mL). Thereafter,
values continuously decreased independently of further ATG
administration. Elevated levels of PCT were also detected in
patients undergoing liver transplant and immunosuppression
without ATG therapy; however, peak levels reached only 13.9
ng/mL, again occurring on the first postoperative day (Table
1).
In the group of patients undergoing liver resection, the median
PCT on the first postoperative day was 0.6 ng/mL (minimum
0.1 ng/mL, maximum 2.5 ng/mL) and PCT levels peaked on
the second postoperative day (median 1.1 ng/mL, minimum
0.3 ng/mL, maximum 3.6 ng/mL) and then decreased to the
normal range (Figure 1).
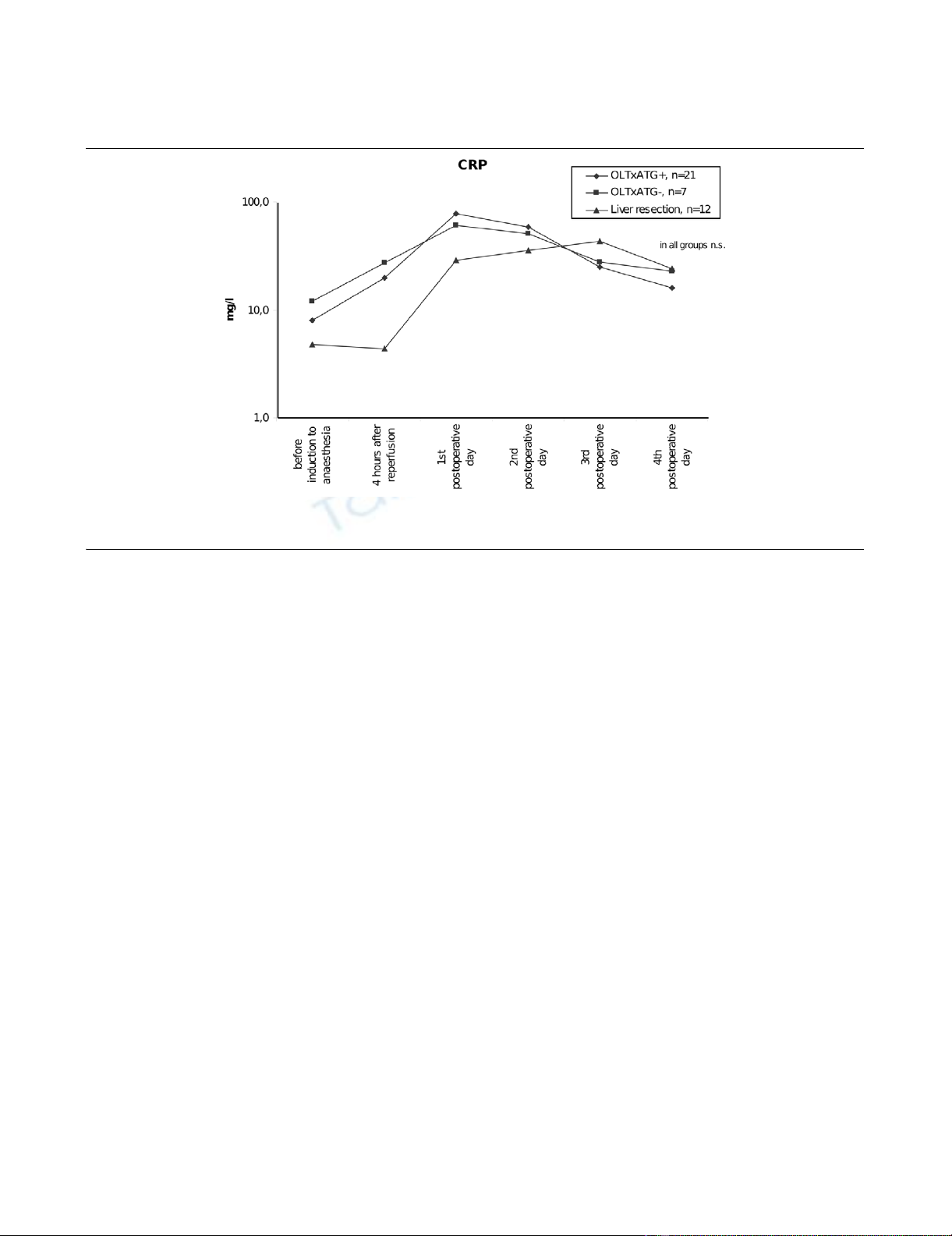
CRP levels were elevated in patients with OLTx and immuno-
suppressive therapy with ATG on postoperative days 1 and 2
after reperfusion. The maximum levels were observed on the
first postoperative day and then decreased. CRP levels also
increased over the first 2 days postoperatively in patients with
OLTx without ATG. In patients with liver resection, we found
the maximum levels of CRP on the second postoperative day,
with a subsequent decrease on the fourth postoperative day
Available online http://ccforum.com/content/11/6/R131
Page 3 of 5
(page number not for citation purposes)
Figure 1
Procalcitonin (PCT) serum levels in patients after orthotopic liver transplantation (OLTx) with and without anti-thymocyte globulin (ATG) therapy and after liver resectionProcalcitonin (PCT) serum levels in patients after orthotopic liver transplantation (OLTx) with and without anti-thymocyte globulin (ATG) therapy and
after liver resection.
Table 1
Serum levels of PCT and CRP in patients after OLTx with and without ATG administration and after liver resection
OLTx with ATG,
median (min-max)
n = 21
Before
induction to
anesthesia
4 hours after
reperfusion 8 hours after
reperfusion 1st
postoperative
day
2nd
postoperative
day
3rd
postoperative
day
4th
postoperative
day
PCT, ng/mL 0.4
(0.1–1.24) 12.2
(1.4–49.7) 43.8
(8.64–206.8) 53.0
(7.9–249.1) 25.1
(3.4–187.1) 15.5
(2.2–82.8) 8.5
(1.16–23.0)
CRP, mg/L 8.0
(0.0–61.8) 19.8
(1.4–53.0) 28.5
(5.40–131.0) 78.0
(22.0–181.0) 59.0
(11.7–145.0) 25.0
(4.2–87.0) 16.0
(2.2–86.0)
OLTx without
ATG
administration,
median (min-max)
n = 7
Before
induction to
anesthesia
4 hours after
reperfusion 8 hours after
reperfusion 1st
postoperative
day
2nd
postoperative
day
3rd
postoperative
day
4th
postoperative
day
PCT, ng/mL 0.4 (0.1–1.1) 3.0 (0.8–3.8) 3.6 (1.1–11.6) 3.0 (1.4–13.9) 1.6 (1.0–8.8) 1.0 (0.6–4.4) 1.0 (0.2–3.1)
CRP, mg/L 12.0
(0.0–29.5) 27.4
(8.0–90.0) 54.0
(21.0–112.0) 61.0
(40.0–148.0) 51.0
(22.0–90.0) 28.0
(11.0–55.0) 23.0
(6.3–47.0)
Liver resection,
median (min-max)
n = 12
Before
induction to
anesthesia
After admission to
intensive care unit 1st
postoperative
day
2nd
postoperative
day
3rd
postoperative
day
4th
postoperative
day
PCT, ng/mL 0.2 (0.1–0.7) 0.2 (0.1–0.8) 0.6 (0.1–2.5) 1.1 (0.3–3.6) 0.9 (0.2–3.6) 0.6 (0.2–1.8)
CRP, mg/L 4.8
(0.0–27.0) 4.4
(0.0–19.0) 29.0
6.0–80.0) 35.7
(12.0–142.0) 43.0
(7.0–173.0) 24.0
(5.0–144.0)
ATG, anti-thymocyte globulin; CRP, C-reactive protein; min-max, minimum to maximum; OLTx, orthotopic liver transplantation; PCT, procalcitonin.
Critical Care Vol 11 No 6 Zazula et al.
Page 4 of 5
(page number not for citation purposes)
(Table 1). In contrast to PCT, no differences were found in
CRP levels in any of the groups of patients (Figure 2). None of
the patients in this study had any evidence of rejection over the
first month after transplantation and there were no septic com-
plications during this period either.
Discussion
The role of PCT under physiological conditions and in sepsis
has not been fully elucidated yet. Experimental and clinical
studies imply that PCT might act as a toxic factor in severe
bacterial inflammation [10]. Regarding its place of origin, PCT
is a rather ubiquitous molecule [11-13]. The absence of PCT
production in the model of hepatectomized baboons suggests
a primary role for the liver as a source of PCT production dur-
ing endotoxin shock [14].
Our results seem to illustrate the link between the type of
immunosuppressive drug and induction of PCT production.
Transient elevation of PCT due to the immunosuppressive
therapy in kidney or liver transplant patients has been
described in other studies [5,6,8,9]. In those studies, as well
as in our cohort of patients, no systemic bacterial infection has
been detected. Interestingly, in each group of patients, a dif-
ferent immunosuppressive therapy was used: ATG, anti-CD3
monoclonal antibody, and systemic corticosteroids.
What is important from the clinical point of view? If there is a
systemic bacterial infection present in a patient, one of the
most important issues in the monitoring of PCT is its dynamics.
In our study, in both groups of patients receiving immunosup-
pressive therapy, an elevated level of PCT was found, espe-
cially in the group of ATG-treated patients. The PCT levels
reached their peak values on the first postoperative day and
ceased thereafter in all patients. None of the patients dis-
played any sign of systemic bacterial infection. These results
correlate very well with the findings of Kuse and colleagues
[6,8] in a group of patients after liver transplant. Similar results
have been found by Sabat and colleagues [9] in patients after
liver transplant. The study of Fazakas and colleagues [15] doc-
umented only a mild elevation of PCT levels immediately after
graft reperfusion in patients after liver transplantation without
OKT3 (monoclonal antibody that specifically reacts with the T
cell receptor-CD3 complex on the surface of circulating
human T cells) or ATG therapy. Thus, it is noticeable that very
high levels of PCT (in the range of hundreds of nanograms),
even if elevated only transiently, are not connected with the
presence of systemic bacterial infection.
The regulatory processes connected with such high levels of
PCT are complicated to address, and, at present, only hypoth-
eses are available. Kuse and colleagues [6,8] speculated that
systemic cytokine release induced by OKT3/ATG administra-
tion could lead to increased enteral permeability with endo-
toxin translocation causing the PCT increase. In contrast to the
findings of this study are those of Redl and colleagues [16],
who assessed the correlation of PCT levels and tumor necro-
sis factor in an Escherichia coli model in baboons. They did
not find any correlation between PCT and tumor necrosis fac-
tor levels. Our results support the study of Sabat and col-
leagues [9] with patients after kidney transplantation, in which
the highest PCT levels were found in patients with ATG ther-
apy. What is the reason for this? Polyclonal ATG is produced
by immunization of rabbits with the human Jurkat T cell line.
One of the molecules expressed in the Jurkat T cell line is intra-
Figure 2
C-reactive protein (CRP) serum levels in patients after orthotopic liver transplantation (OLTx) with and without anti-thymocyte globulin (ATG) therapy and after liver resectionC-reactive protein (CRP) serum levels in patients after orthotopic liver transplantation (OLTx) with and without anti-thymocyte globulin (ATG) therapy
and after liver resection. n.s., not significant.
Available online http://ccforum.com/content/11/6/R131
Page 5 of 5
(page number not for citation purposes)
cellular adhesion molecule-1 (CD54), which is involved in the
process of inflammation, and its expression is induced by
ischemia. The liver and mononuclear cells could represent a
potential source of PCT production triggered by ATG therapy
and cold ischemia during perioperative management. Con-
cerning these findings, we suspect that, in the case of polyclo-
nal antibodies, more binding epitopes and more targets for the
initiation of the process of inflammation are present.
Conclusion
The type of immunosuppressive therapy influences PCT
serum levels in patients after OLTx. Administration of pan-T-
cell antibodies to patients with OLTx is associated with a sig-
nificant increase in serum PCT levels, with peak values on the
first postoperative day. PCT rises in the absence of any clinical
and microbiological evidence of sepsis. Further studies are
needed to elucidate the mechanisms responsible for the PCT
production.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
RZ helped conceive, design, and carry out the study and
shares responsibility for its outline. MP helped conceive,
design, and carry out the study, shares responsibility for its
outline, and performed laboratory analyses. TT and EK per-
formed the literature search, identified the relevant studies to
be included in the analysis, and compiled the data for the
study. All authors contributed to the writing of the manuscript
and approved of its final version.
References
1. Reinhart K, Meisner M, Brunkhorst FM: Markers for sepsis diag-
nosis: what is useful? Crit Care Clin 2006, 22:503-519.
2. Uzzan B, Cohen R, Nicolas P, Cucherat M, Perret GY: Procalci-
tonin as a diagnostic test for sepsis in critically ill adults and
after surgery or trauma: a systematic review and meta-analy-
sis. Crit Care Med 2006, 34:1996-2003.
3. Jensen JU, Heslet L, Jensen TH, Espersen K, Steffensen P, Tvede
M: Procalcitonin increase in early identification of critically ill
patients at high risk of mortality. Crit Care Med 2006,
34:2596-2602.
4. Eberhard OK, Langefeld I, Kuse ER: Procalcitonin in the early
phase after renal transplantation-will it add to diagnostic
accuracy. Clin Transplant 1998, 12:206-211.
5. Kunz D, Pross M, König W, Lippert H, Manger T: Diagnostic rele-
vance of procalcitonin, IL-6 and cellular immune status in the
early phase after liver transplantation. Transplant Proc 1998,
30:2398-2399.
6. Kuse ER, Langefeld I, Jaeger K, Kulpmann WR: Procalcitonin in
fever of unknown origin after liver transplantation: a variable to
differentiate acute rejection from infection. Crit Care Med
2000, 28:555-559.
7. Stríz I, Jaresová M, Lácha J, Sedlácek J, Vítko S: MRP 8/14 and
procalcitonin serum levels in organ transplantations. Ann
Transplant 2001, 6:6-9.
8. Kuse ER, Jaeger K: Procalcitonin increase after anti-CD3 mon-
oclonal antibody therapy does not indicate infectious disease.
Transpl Int 2001, 14:55.
9. Sabat R, Höflich C, Döcke WD, Oppert M, Kern F, Windrich B,
Rosenberger C, Kaden J, Volk HD, Reinke P: Massive elevation
of procalcitonin plasma levels in the absence of infection in
kidney transplant patients treated with pan-T-cell antibodies.
Intensive Care Med 2001, 27:987-991.
10. Nylen ES, Whang KT, Snider RH Jr, Steinwald PM, White JC,
Becker KL: Mortality is increased by procalcitonin and
decreased by an antiserum reactive to procalcitonin in experi-
mental sepsis. Crit Care Med 1998, 26:1001-1006.
11. Linscheid P, Seboek D, Schaer DJ, Zulewski H, Keller U, Müller B:
Expression and secretion of procalcitonin and calcitonin gene-
related peptide by adherent monocytes and by macrophage-
activated adipocytes. Crit Care Med 2004, 32:1715-1721.
12. Silomon M, Bach F, Ecker D, Graeter T, Grundmann U, Larsen R:
Procalcitonin after extracorporeal circulation. Synthesis in the
hepatosplanchnic region. Anaesthesist 1999, 48:395-398.
13. Meisner M, Müller V, Khakpour Z, Toegel E, Redl H: Induction of
procalcitonin and proinflammatory cytokines in an anhepatic
baboon endotoxin shock model. Shock 2003, 19:187-190.
14. Redl H, Schiesser A, Tögel E, Assicot M, Bohuon C: Possible role
of TNF on procalcitonin release in a baboon model of sepsis.
Shock 2001, 16:25-27.
15. Fazakas J, Gondos T, Varga M, Sarvary E, Horovitz P, Perner F:
Analysis of systemic and regional procalcitonin serum levels
during liver transplantation. Transpl Int 2003, 16:465-470.
16. Redl H, Schlag G, Tögel E, Assicot M, Bohuon C: Procalcitonine
release patterns in a baboon model of trauma and sepsis:
relationship to cytokines and neopterin. Crit Care Med 2000,
28:3659-3663.
Key messages
• The type of immunosuppressive therapy influences pro-
calcitonin (PCT) serum levels in liver transplant patients.
• Administration of anti-thymocyte globulin (ATG) is a
powerful stimulus for PCT synthesis and release.
• The transient high PCT values in orthotopic liver trans-
plantation patients with and without ATG treatment are
not caused by bacterial infection.
• There is still limited knowledge on the mechanisms of
PCT synthesis and release.



![PET/CT trong ung thư phổi: Báo cáo [Năm]](https://cdn.tailieu.vn/images/document/thumbnail/2024/20240705/sanhobien01/135x160/8121720150427.jpg)






















%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)