CAS E REP O R T Open Access
A role of
18
F-fluorodeoxyglucose positron
emission/computed tomography in a strategy for
abdominal wall metastasis of colorectal mucinous
adenocarcinoma developed after laparoscopic
surgery
Kimihiko Funahashi
*
, Mitsunori Ushigome, Hironori Kaneko
Abstract
Metastasis to the abdominal wall including port sites after laparoscopic surgery for colorectal cancer is rare.
Resection of metastatic lesions may lead to greater survival benefit if the abdominal wall metastasis is the only
manifestation of recurrent disease. A 57-year-old man, who underwent laparoscopic surgery for advanced
mucinous adenocarcinoma of the cecum 6 years prior, developed a nodule in the surgical wound at the lower
right abdomen. Although tumor markers were within normal limits, the metastasis to the abdominal wall and
abdominal cavity from the previous cecal cancer was suspected. An abdominal computed tomography scan did
not provide detective evidence of metastasis.
18
F-fluorodeoxyglucose positron emission/computed tomography
(
18
F-FDG PET/CT) was therefore performed, which demonstrated increased
18
F-fluorodeoxyglucose uptake
(maximum standardized uptake value: 3.1) in the small abdominal wall nodule alone. Histopathological examination
of the resected nodule confirmed the diagnosis of metastatic mucinous adenocarcinoma. Prognosis of intestinal
mucinous adenocarcinoma is reported to be poorer than that of non-mucinous adenocarcinoma. In conclusion,
this case suggests an important role of
18
F-FDG PET/CT in early diagnosis and decision-making regarding therapy
for recurrent disease in cases where a firm diagnosis of recurrent colorectal cancer is difficult to make.
Background
Metastasis to the abdominal wall including port sites after
laparoscopic surgery for colorectal carcinoma (CRC) is
rare. Recently the rate was reported as 1.3% in a rando-
mized clinical trial by the Colon Cancer Laparoscopic or
Open Resection Study Group [1] and 2.4% in the CLAS-
SIC trial [2]. Although the prognosis is not clearly defined
in the literature, resection of metastatic lesions may lead
to greater survival benefit if the abdominal wall metastasis
is the only manifestation of recurrent disease. However, it
can be difficult to diagnose a lesion in the abdominal wall
as recurrence of disease on the basis of clinical characteris-
tics alone. Approximately between 5% to 15% of CRCs are
mucinous adenocarcinomas [3-7]. Patients with colorectal
mucinous adenocarcinoma are reported to have a poorer
prognosis compared to patients with non-mucinous ade-
nocarcinoma because the greater frequency of lymph node
involvement and peritoneal dissemination seen with muci-
nous adenocarcinoma [7-10]. Therefore, Patients with
mucinous adenocarcinoma should be followed carefully
after surgery, and receive rapid diagnosis and treatment if
recurrence is suspected. We report a case in which
18
F-
fluorodeoxyglucose positron emission/computed tomogra-
phy (
18
F-FDG PET/CT) was very useful for early diagnosis
and planning a theraupetic strategy for a case of mucinous
adenocarcinoma metastasis at a laparoscopic port site.
Case presentation
A 57-year-old man received curative laparoscopic ileoce-
cal resection and lymph node dissection for carcinoma
of the cecum in May 2004. Morphologically, the tumor
* Correspondence: kingkong@med.toho-u.ac.jp
Department of Gastroenterological Surgery, Toho University Medical Center,
Omori Hospital, 6-11-1 Omori nishi, Otaku, Tokyo, 143-8541, Japan
Funahashi et al.World Journal of Surgical Oncology 2011, 9:28
http://www.wjso.com/content/9/1/28 WORLD JOURNAL OF
SURGICAL ONCOLOGY
© 2011 Funahashi et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative
Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and
reproduction in any medium, provided the original work is properly cited.
was type I (45 mm by 30 mm). The histological exami-
nation revealed a mucinous adenocarcinoma which
invaded the cecal subserosa. Tumor cells were not iden-
tified histologically in the 20 regional lymph nodes, sur-
gical margins, lymph vessels, or veins of the surgical
specimens (pT3 N0 M0). The patient was subsequently
followed at our hospital and treated with oral 5-fluor-
ouracil. In February 2008, the patient discovered a
nodule in the incision site in the lower right abdomen.
A 2-cm, firm, ill-defined, tender mass was palpable in
the incision site, and was suspected to be a recurrence
of the cecal mucinous adenocarcinoma. However, the
levels of carcinoembryonic antigen (CEA) and carbohy-
drate antigen 19-9 (CA19-9) were within normal limits
(CEA: 4.7 ng/dl, CA19-9: 16.2 U/ml). In November
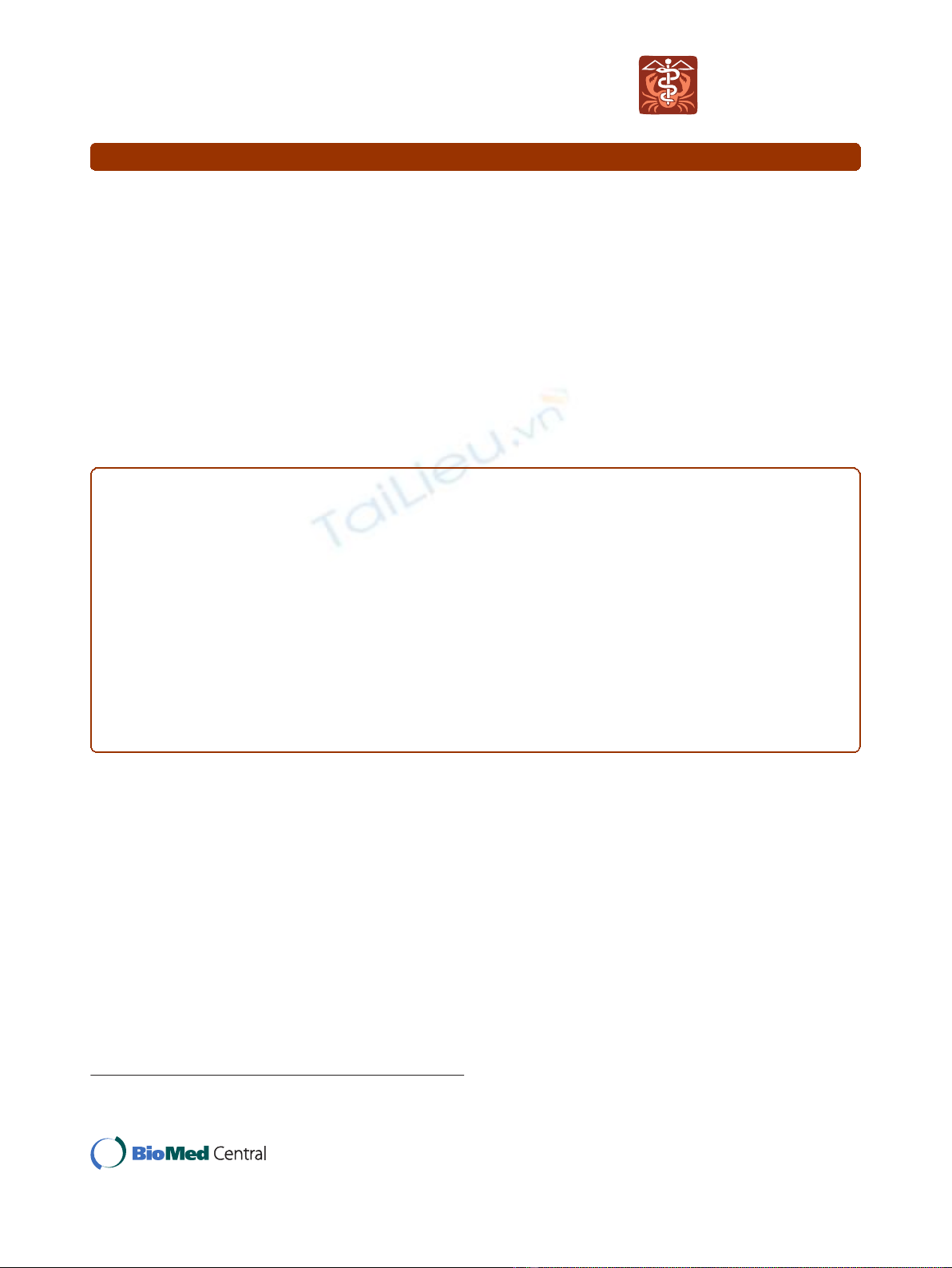
2008, an abdominal computed tomography (CT) scan
revealed a small nodule in the abdominal wall, which
was difficult to interpret as metastasis of the cecal can-
cer (Figure 1). 18F-fluorodeoxyglucose (
18
F-FDG) posi-
tron emission/computed tomography (PET/CT) was
performed in January 2009. The CT scan was performed
first, from head to pelvic floor using 3.3-mm section
thickness. Immediately after the CT scan, a PET scan
was performed using the identical transverse field of
view and section thickness as that of the CT scan. For
the PET scan, the patient, whose blood glucose level
was 103 mg/dl, received 181.8 MBq of
18
F-FDG intra-
verously. Data acquisition was performed within 20 min
after injection using an integrated PET/CT system (Emi-
nence SOPHIA; Shimadzu Corporation, Kyoto, Japan).
PET image data sets were reconstructed by
137
caesium
for attenuation correction, and coregistered images were
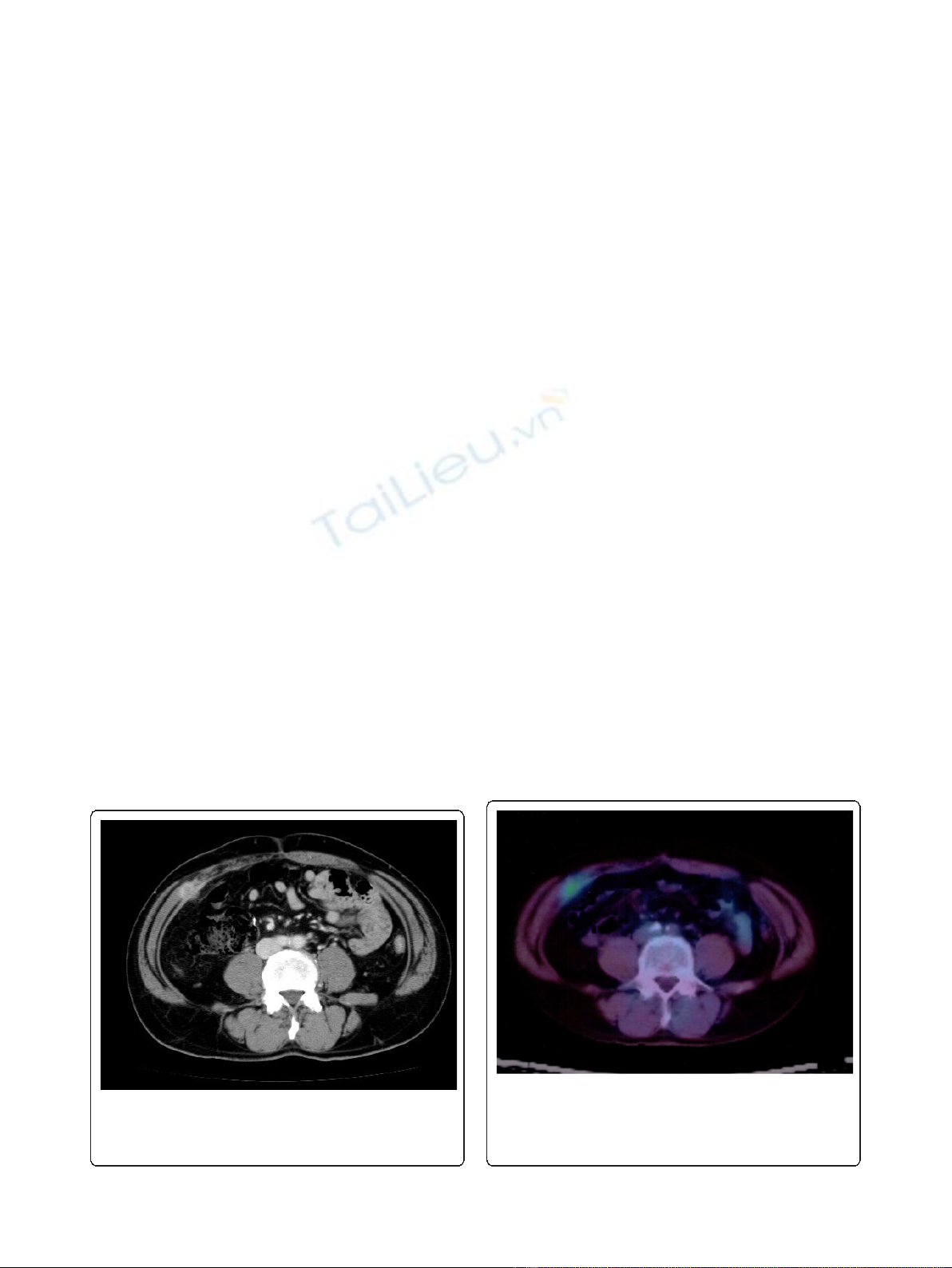
displayed. The PET/CT scan demonstrated increased
18
F-
FDG uptake (maximum standardized uptake value: 3.1)
in the small abdominal nodule, but no further metastases
in distant organs, peritoneum, or lymph nodes. The small
nodule was diagnosed as a solitary metastasis of the cecal
cancer at the previous port site (Figure 2). The nodule was
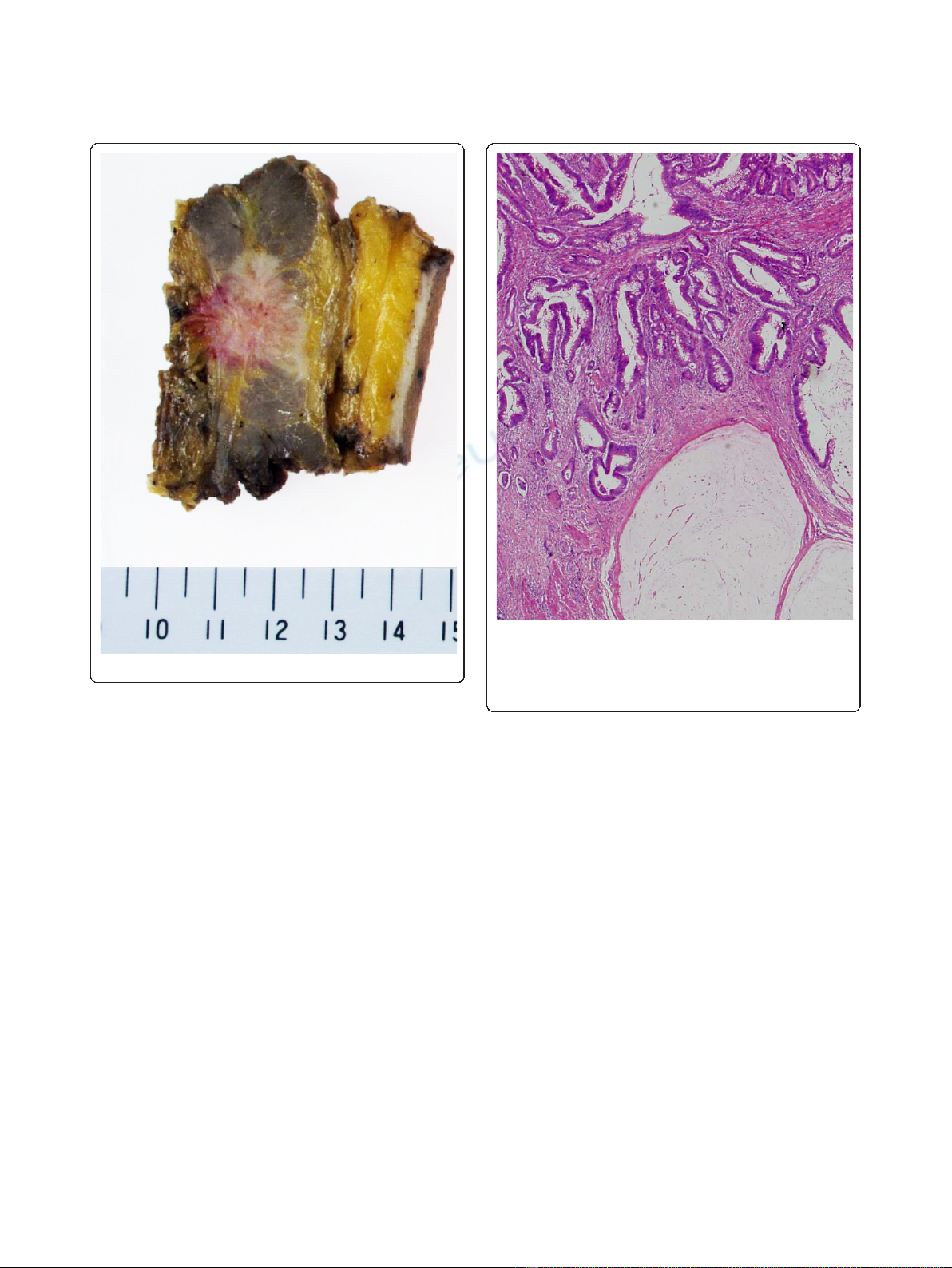
resected in February 2009. The tumor was located in the
abdominal wall, slightly exposed to the abdominal cavity.
There was no gross evidence of metastasis in the abdom-
inal cavity and cytological examination identified no
tumor cells in the ascitic fluid. The tumor was identified
as a metastatic lesion on the basis of histological findings
(Figures 3, 4 and 5). No recurrence developed during 24-
months postsurgical follow up.
Discussion
Port site metastasis after laparoscopic surgery for CRC is
rare, reported as 0.71-1% in the literature [11-16].
Recently the rate was reported as 1.3% in a randomized
clinical trial by the Colon Cancer Laparoscopic or Open
ResectionStudyGroup[1]and2.4%intheCLASSIC
trial [2]. Several factors that may contribute to abdom-
inal wall metastasis have been proposed [17], but it was
impossible to identify a cause in this case. The operating
record indicated that a wound drape had been used to
prevent the implantation of tumor cells during surgery;
clinico-pathologically, the depth of invasion of the pri-
mary tumor was confined to the intestinal wall and no
vascular invasion was identified, and there were no post-
operative complications.
Early resection of the metastatic lesion may lead to
greater survival benefit, but early confirmation of meta-
static disease on the basis of clinical characteristics
alone is challenging.
18
F-FDG PET/CT imaging, which
both structural and functional information provide, is
Figure 1 Abdominal computed tomography scan.Abdominal
computed tomography scan on November 2008 revealed a small
nodule in the abdominal wall, which was difficult to interpret as
metastasis of cecal cancer by only computed tomography image.
Figure 2
18
F-fluorodeoxyglucose positron emission/computed
tomography.
18
F-fluorodeoxyglucose positron emission/computed
tomography demonstrated increased
18
F-fluorodeoxyglucose uptake
(maximum standardized uptake value: 3.1) in the small nodule in
the abdominal wall.
Funahashi et al.World Journal of Surgical Oncology 2011, 9:28
http://www.wjso.com/content/9/1/28
Page 2 of 5
used to identify and stage various types of tumors
because of its superiority to traditional imaging for diag-
nosing recurrent disease. In a retrospective comparison
of PET versus PET/CT for the detection of CRC recur-
rence, the sensitivity, specificity and overall accuracy of
PET were 80%, 69% and 75% respectively, compared
with 89%, 92% and 90%, respectively, for PET/CT [18].
Goshen et al [19] reported
18
F-FDG PET/CT was a sen-
sitive tool for the diagnosis of 16 abdominal wall lesions
in 12 CRC patients, who had moderately or well-differ-
entiated adenocarcinoma. Kozugi et al reported that
18
F-
FDG PET was an important tool for the detection of
port site recurrence of colon cancer in a patient who
had elevated serum CEA levels but no metastases
detected using routine radiographic examinations [20].
In addition, Sarikaya et al retrospectively analyzed the
usefulness of PET for patients with CRC and suspected
tumor recurrence, but normal CEA levels, and found
that the overall accuracy of PET was 76.9%, and the
positive predictive value was 84.6%. They concluded that
PET yielded high positive predictive value for recurrence
CRC despite normal CEA levels, and should be consid-
ered early in the evaluation of patients with suspected
tumor recurrence [21].
18
F-FDG PET/CT is useful tool
to help interpret potential malignancies when routine
radiographic examinations are inconclusive. In addition,
we consider that
18
F-FDG PET/CT should be a prere-
quisite examination in patients with suspected recur-
rence of CRC who have normal CEA levels.
18
F-FDG PET/CT imaging, however, does have some dis-
advantages. False-negative findings can occur for several
reasons, including inflammation, small lesions size and dia-
betes. Mucinous adenocarcinoma as a histological type,
regardless of the organs, may result in more false negatives
as well. Sarikaya et al [21] reported that 3 of 5 patients
(60%) with false-negative PET findings had mucinous ade-
nocarcinoma diagnosed histologically. Rodriguez-Fernandez
et al [22] and Sun L et al [23] reported false-negative results
in patients with mucinous adenocarcinoma of the gallblad-
der and gastric cancer, respectively. For detection of gall-
bladder recurrence
18
F-FDG PET scan showed a sensitivity
of 80%, a specificity of 82%, and positive and negative pre-
dictive values of 67% and 90%, respectively. The single
false-negative result was a patient with mucinous adenocar-
cinoma. For detection of gastric cancer recurrence, the
accuracy of
18
F-FDG PET/CT scan was 82.6%, and positive
and negative predictive values were 85.7% and 77.7%,
Figure 3 Resected specimen.
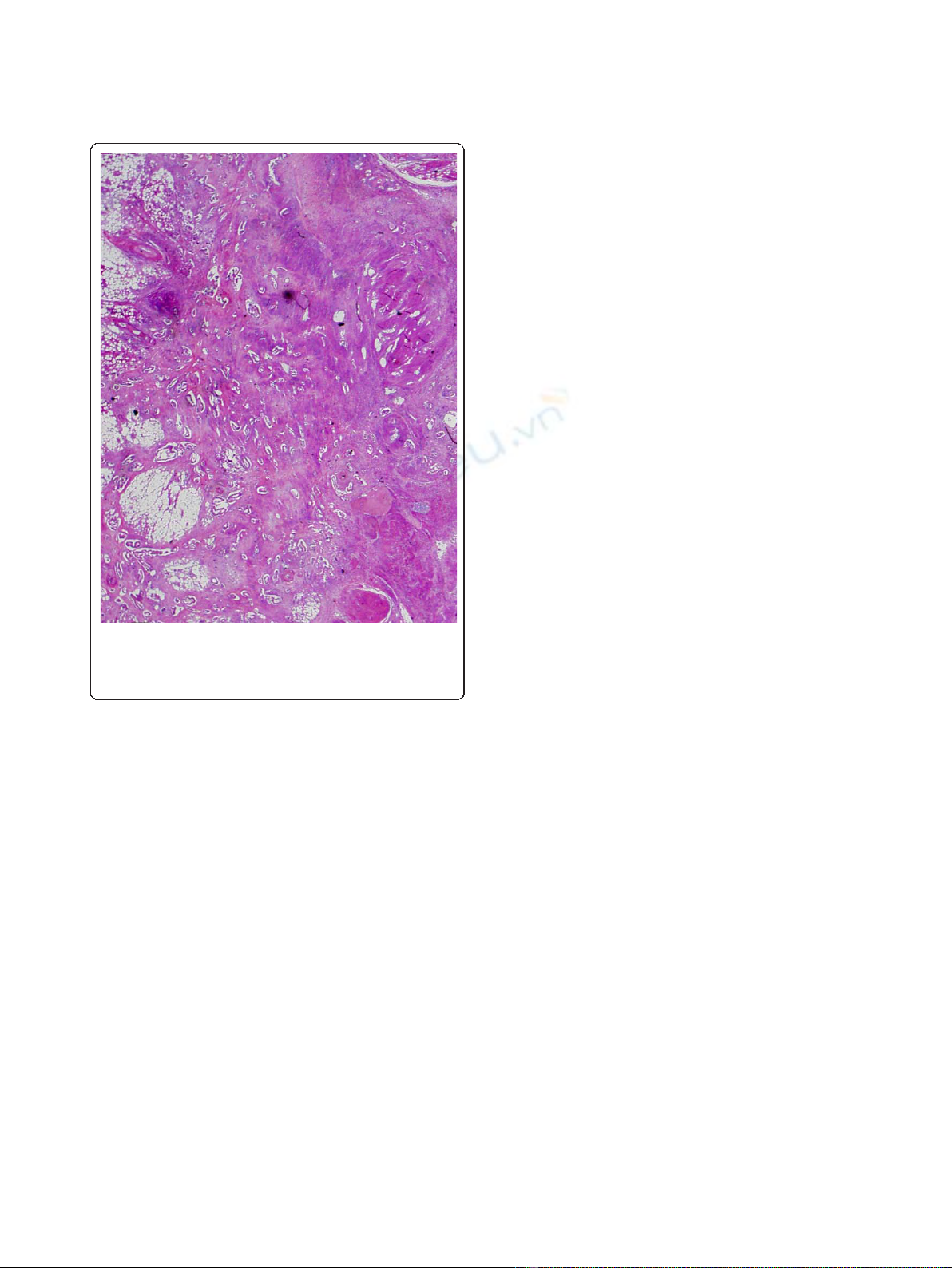
Figure 4 Pathological findings. Primary tumor. The histological
examination revealed mucinous adenocarcinoma invading into the
subserosa. Tumor cells in the regional lymph nodes, surgical
margins, lymph vessels and veins were not identified histologically
in the specimen (pT3 N0 M0).
Funahashi et al.World Journal of Surgical Oncology 2011, 9:28
http://www.wjso.com/content/9/1/28
Page 3 of 5
respectively. The two false-negative in patients with muci-
nous adenocarcinoma as shown in these reports, and in
our case study it can be difficult to detect lesions of muci-
nous adenocarcinoma by PET scan and
18
F-FDGPET/CT
scan can be very useful in early diagnosis and therapeutic
management.
Mucinous adenocarcinomas have a biological behavior
that involves more lymph nodes at diagnosis and the
greater frequency of peritoneal dissemination when com-
pared to non-mucinous adenocarcinomas [7-10]. Recently,
treatment with FOLFOX (Folinic acid + Fluorouracil +
Oxaliplatin) or FOLFIRI (Folinic acid + Fluorouracil + Iri-
notecan) has been considered useful to obtain better pro-
gression-free survival for unresectable colorectal
recurrence. However, there is no doubt that early com-
plete resection of the metastatic lesion could lead to even
greater survival benefit.
18
F-FDG PET/CT scan can play
an important role in selecting among patients with recur-
rence those who may obtain greater survival benefit.
Conclusion
In the case we presented
18
F-FDG PET/CT scan was very
useful in early diagnosis and therapeutic management for
recurrence of mucinous adenocarcinoma after laparo-
scopic surgery for CRC. Mucinous adenocarcinomas may
contribute to a higher rate of false-negative results, but
does not decrease the usefulness of this diagnostic tool.
18
F-FDG PET/CT imaging, which provide both func-
tional and anatomical information and correctly stages
recurrence disease should be considered early in the eva-
luation of patients with suspected recurrence of CRC.
Consent
Written informed consent was obtained from the patient
for publication of this case report and any accompany-
ing image. A copy of the written consent is available for
review by the Editor-in Chief of this journal.
Abbreviations
CRC: colorectal carcinoma;
18
F-FDG PET/CT:
18
F-fluorodeoxyglucose positron
emission/computed tomography;
18
F-FDG:
18
F-fluorodeoxyglucose; PET/CT:
positron emission/computed tomography; CEA: carcinoembryonic antigen;
CA19-9: carbohydrate antigen 19-9; CT: computed tomography; PET: positron
emission tomography; FOLFOX: Folinic acid + Fluorouracil + Oxaliplatin;
FOLFIRI: Folinic acid + Fluorouracil + Irinotecan;
Authors’contributions
MU was an assistant of the operation. HK is a chairman of the department
of gastroenterological surgery, Toho University Medical Center, Omori
Hospital. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Received: 3 October 2010 Accepted: 28 February 2011
Published: 28 February 2011
References
1. The Colon Cancer Laparoscopic or Open resection Study Group, Buunen M,
Veldkamp R, Hop WC, Kuhry E, Jeekel J, Haglind E, Påhlman L, Cuesta MA,
Msika S, Morino M, Lacy A, Bonjer HJ: Survival after laparoscopic surgery
versus open surgery for colon cancer: long-term outcome of a
randmised cilinical trial. Lancet Oncol 2009, 10:44-52.
2. Jayne DG, Thorpe HC, Copeland J, Quirke P, Brown JM, Guillou PJ: Five-year
follow -up of the medical research council CLASSIC trial of
laparoscopically assisted versus open surgery for colorectal cancer. Br J
Surg 2010, 97:1638-1645.
3. Symonds DA, Vickery AL: Mucinous carcinoma of the colon and rectum.
Cancer 1976, 37:1891-1900.
4. Fante R, Benatti P, di Gregorio C, De Pietri S, Pedroni M, Tamassia MG,
Percesepe A, Rossi G, Losi L, Roncucci L, Ponz de Leon M: Colorectal
carcinoma in different age groups. A population-based investigation. Am
J Gastroenterol 1997, 92:1505-1509.
5. Yamamoto S, Mochizuki H, Hase K, Yamamoto T, Ohkusa Y, Yokoyama S,
Ushitani Y, Tamakuma S: Assessment of clinicopathologic features of
colorectal mucinous adenocarcinoma. Am J Surg 1993, 166:257-261.
6. Wu CS, Tung S, Chen Pc, Kuo YC: Clinicopathological study of colorectal
mucinous carcinoma in Taiwan: A multivariate study. J Gastroenterol
Hepatol 1996, 11:77-81.
7. Nozoe T, Anai H, Nasu S, Sugimachi K: Clinicopathological characteristics
of mucinous carcinoma of the colon and rectum. J Surg oncol 2000,
75:103-107.
8. Maksimovic S: Survival rates of patients with mucinous adenocarcinoma
of the colorectum. Med Arh 2007, 61:26-29.
9. Kanemitsu Y, Kato T, Yasui K, Morimoto T, Shimizu Y, Kodera Y,
Yamamura Y: Survival after curative resection for mucinous
adenocarcinoma of the colorectum. Dis Colon Rectum 2003, 46:160-167.
Figure 5 Pathological findings. Metastatic tumor. The tumor was
located in the abdominal wall, slightly exposed to the abdominal
cavity. Clinico-pathological findings showed the tumor was
identified as a metastasis from cecal carcinoma.
Funahashi et al.World Journal of Surgical Oncology 2011, 9:28
http://www.wjso.com/content/9/1/28
Page 4 of 5
10. Green JB, Timmcke AE, Mitchell WT, Hicks TC, Gathright JB Jr, Ray JE:
Mucinous carcinoma -just another colon cancer? Dis Colon Rectum 1993,
36:49-54.
11. Ziprin P, Ridgway PF, Peck DH, Darzi AW: The theories and realities of
port-site metastases: a critical appraisal. J Am Coll Surg 2002, 195:395-408.
12. Zmora O, Gervaz P, Wexner SD: Trocar site recurrence in laparoscopic
surgery for colorectal cancer. Surg Endosc 2001, 15:788-793.
13. Lacy AM, Delgado S, Garcia-Valdecasas JC, Castells A, Pique JM, Grande L,
Fuster J, Targarona EM, Pera M, Visa J: Port site metastases and recurrence
after laparoscopic colectomy; a randomized trial. Surg Endosc 1998,
12:1039-1042.
14. Milsom JW, Böhm B, Hammerhofer KA, Fazio V, Steiger E, Elson P: A
prospective, randomized trial comparing laparoscopic versus
conventional techniques in colorectal cancer surgery: a preliminary
report. J Am Coll Surg 1998, 187:46-54.
15. Franklin ME Jr, Rosenthal D, Abrego-Medina D, Dorman JP, Glass JL,
Norem R, Diaz A: Prospective comparison of open vs laparoscopic colon
surgery for carcinoma: five-year results. Dis Colon Rectum 1996, 39(10
suppl):s35-46.
16. Fleshman JW, Nelson H, Peters WR, Kim HC, Larach S, Boorse RR,
Ambroze W, Leggett P, Bleday R, Stryker S, Christenson B, Wexner S,
Senagore A, Rattner D, Sutton J, Fine AP: Early results of laparoscopic
surgery for colorectal cancer; retrospective analysis of 372 patients
treated by Clinical Outcomes of Surgical Therapy (COST) Study Group.
Dis Colon Rectum 1996, 39(10 suppl):s53-58.
17. Curet MJ: Port site metastases. Am J Surg 2004, 187:705-712.
18. Votrubova J, Belohlavek O, Jaruskova M, Oliverius M, Lohynska R, Trskova K,
Sedlackova E, Lipska L, Stahalova V: The role of FDG-PET/CT in the
detection of recurrence colorectal cancer. Eur J Nucl med Mol Imaging
2006, 33:779-784.
19. Goshen E, Davidson T, Aderka D, Zwas ST: PET/CT detects abdominal wall
and port site metastases of colorectal carcinoma. Br J Radiol 2006,
79:572-577.
20. Kosugi K, Ono M, Saito N, Sugito M, Ito M, Murakami K, Sato K, Kotaka M,
Nomura S, Arai M, Kobatake T: Port site recurrence diagnosed by
positoron emission tomography after laparoscopic surgery for colon
cancer. Hepatogastroenterology 2005, 52:1440-1443.
21. Sarikaya I, Bloomston M, Povoski ST, Zhang J, Hall NC, Knopp MV,
Martin EW Jr: FDG-PET scan in patients with clinically and/or
radiologically suspicious colorectal cancer recurrence but normal CEA.
World J Surg Oncol 2007, 5:64.
22. Rodriguez-Fernandez A, Gomez-Rio M, Llamas-Elvira JM, Ortega-Lozano S,
Ferron-Orihuela JA, Ramia-Angel JM, Mansilla-Rosello A, Martinez-del-
Valle MD, Ramos-Font C: Positron-emission tomography with fluorine-18-
fluoro-2- deoxy-D-glucose for gallbladder cancer diagnosis. Am J Surg
2004, 188:171-175.
23. Sun L, Su XH, Guan YS, Pan WM, Luo ZM, Wei JH, Wu H: Clinical role of
18F-fluorodeoxyglucose positron emission tomography/computed
tomography in post-operative follow up of gastric cancer: initial results.
World J Gastroenterol 2008, 14:4627-4632.
doi:10.1186/1477-7819-9-28
Cite this article as: Funahashi et al.: A role of
18
F-fluorodeoxyglucose
positron emission/computed tomography in a strategy for abdominal
wall metastasis of colorectal mucinous adenocarcinoma developed after
laparoscopic surgery. World Journal of Surgical Oncology 2011 9:28.
Submit your next manuscript to BioMed Central
and take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at
www.biomedcentral.com/submit
Funahashi et al.World Journal of Surgical Oncology 2011, 9:28
http://www.wjso.com/content/9/1/28
Page 5 of 5


























%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)