BioMed Central
Page 1 of 5
(page number not for citation purposes)
World Journal of Surgical Oncology
Open Access
Research
Detection of somatostatin receptors in human osteosarcoma
Markos Ioannou*1, Panayiotis J Papagelopoulos2, Ioannis Papanastassiou1,
Ioanna Iakovidou3, Stamatios Kottakis1 and Nikolaos Demertzis1
Address: 1Department of Orthopaedic Surgery, Cancer Hospital, Pireus, Greece, 21st Department of Orthopaedic Surgery, Medical School,
University of Athens, Greece and 3Department of Pathology, Cancer Hospital, Pireus, Greece
Email: Markos Ioannou* - markosioannou@yahoo.gr; Panayiotis J Papagelopoulos - pjp@hol.gr; Ioannis Papanastassiou - jpapa73@yahoo.gr;
Ioanna Iakovidou - yian_kyr@vivodinet.gr; Stamatios Kottakis - dmytas@gmail.com; Nikolaos Demertzis - stavrosmitas@gmail.com
* Corresponding author
Abstract
Background: The location of osteosarcoma in the metaphysis as well as the age of the patients
during the most rapid tumour growth suggest that factors related to skeletal growth are involved
in the pathogenesis of this tumour. In this aspect this study aims to detect somatostatin receptors
in human osteosarcomas and correlate this finding with the clinical outcome of the tumour.
Patients and methods: Immunohistochemical staining for the presence of somatostatin
receptors as well as overall survival and disease free survival rates were retrospectively studied in
twenty-nine osteosarcoma patients.
Results: Four osteosarcomas with several aggressive biologic behaviour expressed somatostatin
receptors. In these four young patients the event free rate was 0% and the overall survival rate was
50% at 4, 3 years. In contrast the event free survival rate of the twenty-five patients with negative
somatostatin receptor status was 72% with an overall survival rate of 76% at 4,3 years.
Conclusion: The present study demonstrates the existence of somatostatin receptors in human
osteosarcoma. Tumours expressing somatostatin receptors seemed to be aggressive with a very
low disease free and overall survival rate compared to osteosarcoma with negative receptor status.
Background
Osteosarcoma is the most common primary malignant
tumour of bone, with the exception of multiple myeloma.
It represents approximately 15% of all biopsy-analyzed
primary bone tumours [1,2]. It is most common in males
and occurs primarily in the second decade of life. The
most common location sites are the metaphysis of bone
[3,4]. The age of the patients, coinciding with the adoles-
cent growth spurt as well as the location of tumour sites
has led to the syllogism that factors related to skeletal
growth are involved in the pathogenesis of this tumour [5-
7]. Previous studies maintain that treatment with growth
hormone and somatostatin affects the growth of osteosa-
rcoma in animal models [8-10]. Somatostatin is believed
to exert antiproliferative effects on tumour cells through
receptor-mediated stimulation of tyrosine phosphatase
and inhibition of other endogenous growth factors, like
growth hormone and insuline-like growth factor 1
[11,12]. In this respect, the presence of somatostatin
receptors in human osteosarcoma may have a diagnostic,
prognostic and therapeutic value [13].
Published: 10 September 2008
World Journal of Surgical Oncology 2008, 6:99 doi:10.1186/1477-7819-6-99
Received: 14 December 2007
Accepted: 10 September 2008
This article is available from: http://www.wjso.com/content/6/1/99
© 2008 Ioannou et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Surgical Oncology 2008, 6:99 http://www.wjso.com/content/6/1/99
Page 2 of 5
(page number not for citation purposes)
In this study we aim to detect somatostatin receptors in
human osteosarcomas and correlate this finding with the
clinical outcome of the tumour.
Patients and methods
Twenty-nine patients with primary osteosarcoma who
were treated at the authors' institution between 1997 and
2006 were included in this study. Fourteen patients were
female and fifteen were male. The average age at the time
of diagnosis was 27.03 years (range 16–49 years) (Table
1). Preoperative evaluation included precision imaging
techniques (plain radiographs, computed tomography
and MRI of the lesion, computed tomography of the chest
and full body scan with Tc99m). Distribution of anatomic
tumour sites was as described in Table 1. The therapeutic
protocol included neoadjuvant chemotherapy in all
patients with high-dose methotrexate [14-16]. During
preoperative chemotherapy one patient died, while we
operated on twenty-eight patients aiming at wide resec-
tion margins.
Twenty-four patients underwent a limb salvage procedure,
while in four patients amputation was the only surgical
option in order to achieve adequate local control.
Disease-free and overall survival was recorded in all
patients (table 2).
Histological specimens were available for all patients and
were reviewed by one experienced pathologist (I.I.). The
resected specimens were sliced coronally or axially or both
to represent the largest portion of the tumour. The slices
were fixed in 10% neutral buffered formaldehyde solution
and embedded separately in paraffin. The sections were
stained with haematoxylin and eosin and were used for
immunohistochemistry. Polyclonal Rabbit Anti-Human
somatostatin was used (Dako, Denmark) [17-19] in order
to detect the presence of somatostatin receptors [20,21].
The study was approved by the Metaxa Anticancer Hospi-
tal Ethical & Scientific Committee.
Table 1: Sex, Age, Location, Surgical Treatment, Outcome and GH receptor status of 29 patients with osteosarcoma.
Sex Age Location (Site) Surgical Treatment Oncologic outcome GH receptor status
1 M 28 Thoracic Spine LSS DOD
(Died On Disease)
2 F 16 Distal femur LSS NED
(No Evident Disease)
3 F 19 Proximal Tibia Amputation DOD +
4 F 17 Proximal Tibia Amputation DOD +
5 F 39 Distal Femur LSS DOD
6 M 28 Distal Femur Amputation NED
7 M 16 Distal Fibula LSS NED
8 M 22 Distal Femur LSS DOD
9 F 18 Distal Femur LSS DOD
10 F 27 Distal Femur LSS NED
11 F 18 Distal Femur Amputation NED
12 F 35 Proximal Tibia LSS NED
13 M 16 Distal Femur LSS NED
14 M 24 Proximal Humerus LSS Disease Progression
(Pulmonary metastases)
+
15 M 18 Proximal Tibia LSS NED
16 M 32 Distal Tibia LSS NED
17 F 34 Hip Died during chemotherapy DOD
18 F 49 Proximal Tibia LSS NED
19 F 24 Distal Femur LSS NED
20 M 44 Proximal Humerus LSS DOD
21 F 39 Distal Femur LSS Disease Progression
(Local recurrence)
22 F 25 Distal Femur LSS NED
23 M 18 Distal Femur LSS NED
24 M 44 Distal Femur LSS NED
25 M 40 Distal Femur LSS NED
26 M 20 Proximal Humerus LSS NED
27 M 30 Proximal Humerus LSS NED
28 M 16 Proximal Tibia LSS Disease Progression
(Pulmonary metastases)
+
29 F 28 Proximal Tibia LSS NED
World Journal of Surgical Oncology 2008, 6:99 http://www.wjso.com/content/6/1/99
Page 3 of 5
(page number not for citation purposes)
Results
Somatostatin receptors were expressed in four osteosar-
coma's that exhibited aggressive features (figure 1 and 2).
These four tumours appeared in young patients (table 3)
with an aggressive biologic behaviour having an event-
free rate of 0% and an overall survival rate of 50% at 4.3
years (table 4). In contrast, the event-free survival rate of
the twenty-five patients with negative growth hormone
receptor status was 72% with an overall survival rate of
76% at 4.3 years.
Case one represents a woman, 19-years-old, with a right
proximal tibia tumour, stage II B+ on Enneking's staging
system [22]. She underwent neoadjuvant chemotherapy
followed by femoral amputation. Histological examina-
tion revealed grade II osteosarcoma with osteoblastic, as
well as chondroblastic areas and 80% tumour necrosis.
Two years later there was a local recurrence in the stump
of the sciatic nerve, which was treated with hip disarticu-
lation and chemotherapy. Four years post-operative, this
patient presented lung metastases, was treated with chem-
otherapy and eventually died after 1 year. In our retrospec-
tive histological study somatostatin receptors were
detected.
Discussion
The use of neoadjuvant chemotherapy in the treatment
protocol of osteosarcoma in the late 70's improved dis-
ease-free survival, giving a cure rate of 60%–70% for
patients with nonmetastatic osteosarcoma of the extremi-
ties at presentation [23-25].
Little is known about the aetiology and pathogenesis of
this tumour. Genetic predisposition, viral aetiology, irra-
diation and alkylating agents have been suggested in the
pathogenesis of osteosarcoma [3,26,27]. Nowadays,
molecular biology seems to be the next step in under-
standing pathogenesis and improving survival of osteosa-
rcoma. Tumour location in the metaphysis as well as the
age of the patients coinciding with the period of rapid
body growth suggest that factors related to skeletal growth
are involved in the pathogenesis of this tumour.
Table 3: Mean Age of patients with positive staining vs. patients
with negative staining for receptors of Growth Hormone.
Patients with Positive
staining for receptors of
Growth Hormone
Patients with Negative
staining for receptors of
Growth Hormone
AGE
(MEAN/RANGE)
19/16–24 years 28,32/16–49 years
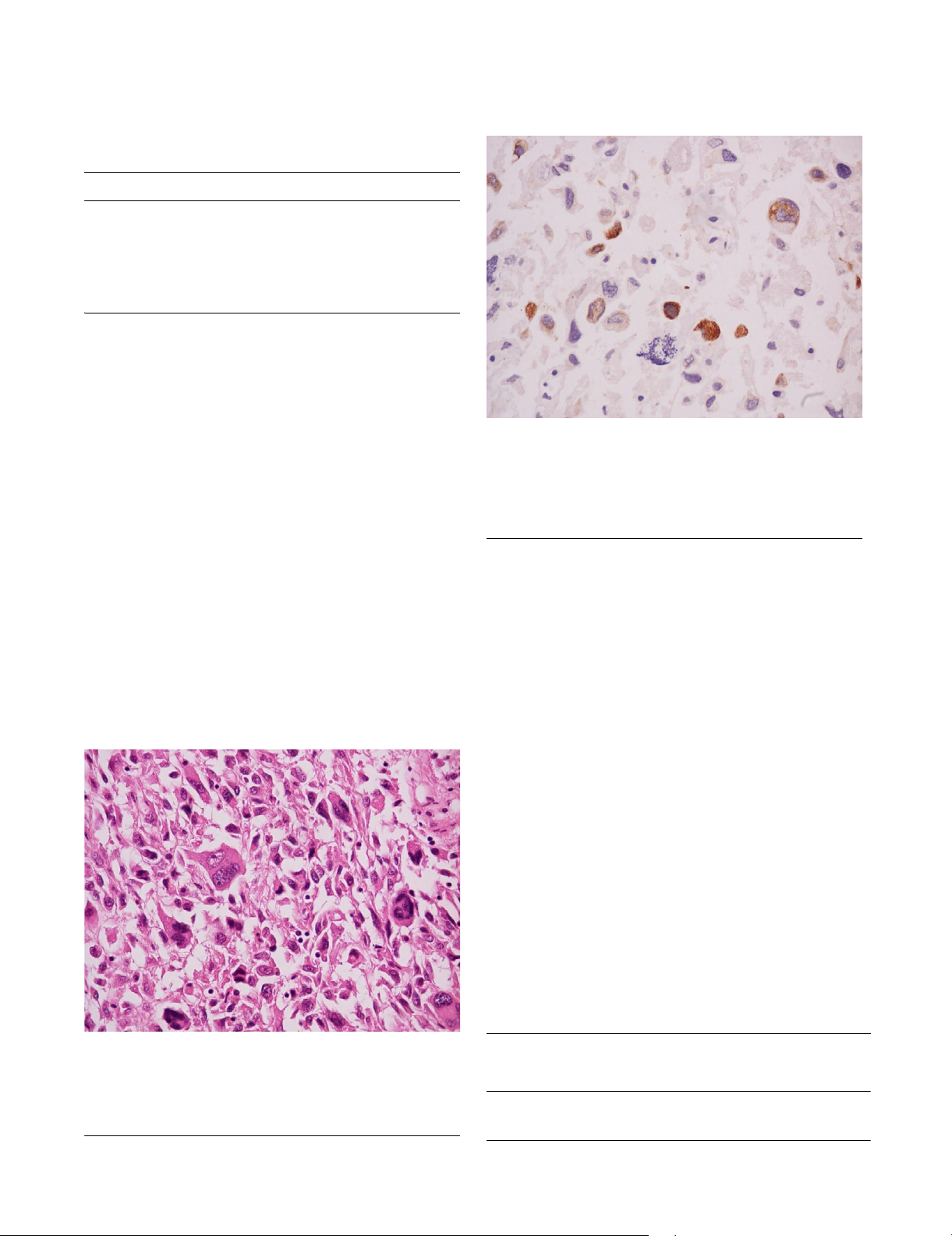
Osteosarcoma somatostatin negative. Magnification ×400Figure 1
Osteosarcoma somatostatin negative. Magnification
×400. This case of an osteosarcoma had no somatostatin
receptors. Immunohistochemistry staining with somatostatin
did not produce any reaction.
Table 2: Disease free and overall survival rate at 4, 48 years, in 29
patients with osteosarcoma.
Frequency Percent
NED
(No Evident Disease)
18 62,0
Disease progression 3 10,4
DOD
(Died On Disease)
827,6
Total 29 100,0
Osteosarcoma somatostatin positive. Magnification ×630Figure 2
Osteosarcoma somatostatin positive. Magnification
×630. In this case staining with somatostatin produced a
reaction appearing with an orange zone around the nuclei.
This case of osteosarcoma is expressing somatostatin recep-
tors.
World Journal of Surgical Oncology 2008, 6:99 http://www.wjso.com/content/6/1/99
Page 4 of 5
(page number not for citation purposes)
Somatostatin is characterized as a hormone which inhib-
its the release of growth hormone from the anterior pitui-
tary gland [28]. The present study demonstrates the
existence of somatostatin receptors in human osteosar-
coma. Further research is necessary to demonstrate the
importance of this finding and its clinical relevance, since
there is also evidence from animal studies that treatment
with growth hormone and somatostatin affects the
growth of osteosarcoma in animal models [8-10]. There is
also one study in pediatric patients having metastatic oste-
osarcoma treated with somatostatin analogue (OncoLar)
which shows that the levels of Insulin-like growth factor-
1 were reduced. However, this study did not yield signifi-
cant clinical results [29].
To our knowledge, there is only one study on humans in
the literature with 18 osteosarcoma patients where the
authors investigated somatostatin receptors by virtue of
scintigraphy. In this study a very high incidence of
patients with somatostatin receptors was found (up to
75%). The authors found higher incidence in non-meta-
static patients and concluded that there is a possible rela-
tion between the somatostatin receptors presence and the
biological behaviour of the tumour. [30]
A limitation to our study is the small number of speci-
mens that were analyzed, which makes statistical analysis
unfeasible; however, because of the novelty of our study
and since the tumours expressing somatostatin receptors
had a more deleterious course with a very low disease-free
and overall survival rate compared to osteosarcoma with
negative receptor status, even though the percentage
(14%) was much lower than that in the Rizzoli study [30],
we believe that this finding should be thoroughly evalu-
ated and investigated with further studies.
Conclusion
In this study we detected somatostatin receptors in human
osteosarcomas. This finding seems to have a prognostic
value, predicating a severe aggressive biologic behaviour
of the tumour as well as possible therapeutic implications.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
MI drafted the manuscript and carried out the design of
the study and performed. II carried out the immunohisto-
chemical studies. PJP, IP and SK participated in the design
and coordination of the study and helped to draft the
manuscript. All authors read and approved the final man-
uscript.
Acknowledgements
The authors would like to thank Panou Christina for text editing
(email:christinepanou@yahoo.com)
References
1. Campanacci M: Bone and soft tissue tumors: clinical features, imaging,
pathology and treatment 2nd edition. Padova: Wein: Springer-Verlag;
1999.
2. Whelan JS: Osteosarcoma. Eur J Cancer 1997, 33:1611-1618. dis-
cussion 1618–1619
3. Huvos AG: Bone tumors: diagnosis, treatment and prognosis 2nd edition.
Philadelphia; London: W.B. Saunders; 1991.
4. Bacci G, Longhi A, Versari M, Mercuri M, Briccoli A, Picci P: Prog-
nostic factors for osteosarcoma of the extremity treated
with neoadjuvant chemotherapy: 15-year experience in 789
patients treated at a single institution. Cancer 2006,
106:1154-1161.
5. Cotterill SJ, Wright CM, Pearce MS, Craft AW: Stature of young
people with malignant bone tumors. Pediatr Blood Cancer 2004,
42:59-63.
6. James RA, Dymock RB: Osteosarcoma associated with acrome-
galy: a case report. Pathology 1976, 8:157-159.
7. Pizzo PA, Poplack DG: Principles and practice of pediatric oncology 4th
edition. Philadelphia; London: Lippincott Williams & Wilkins; 2001.
8. Pinski J, Schally AV, Halmos G, Szepeshazi K, Groot K: Somatosta-
tin analog RC-160 inhibits the growth of human osteosarco-
mas in nude mice. Int J Cancer 1996, 65:870-874.
9. Conzemius MG, Graham JC, Haynes JS, Graham CA: Effects of
treatment with growth hormone and somatostatin on effi-
cacy of diammine [1,1-cyclobutane dicarboxylato (2-)-0,0']-
(SP-4-2) in athymic rats with osteosarcoma. Am J Vet Res 2000,
61:646-650.
10. Khanna C, Prehn J, Hayden D, Cassaday RD, Caylor J, Jacob S, Bose
SM, Hong SH, Hewitt SM, Helman LJ: A randomized controlled
trial of octreotide pamoate long-acting release and carbopl-
atin versus carboplatin alone in dogs with naturally occurring
osteosarcoma: evaluation of insulin-like growth factor sup-
pression and chemotherapy. Clin Cancer Res 2002, 8:2406-2412.
11. Koper JW, Markstein R, Kohler C, Kwekkeboom DJ, Avezaat CJ,
Lamberts SW, Reubi JC: Somatostatin inhibits the activity of
adenylate cyclase in cultured human meningioma cells and
stimulates their growth. J Clin Endocrinol Metab 1992, 74:543-547.
Table 4: Disease free and overall survival rate at 4, 48 years in patients with positive staining vs. patients with negative staining for
receptors of Growth Hormone.
Patients with Positive staining for receptors of Growth
Hormone
(Frequency/Percent)
Patients with Negative staining for receptors of Growth
Hormone
(Frequency/Percent)
NED
(No Evident Disease)
0/0,0 18/72,0
Disease progression 2/50,0 1/4,0
DOD
(Died On Disease)
2/50,0 6/24,0
Total 4/100,0 25/100,0
Publish with BioMed Central and every
scientist can read your work free of charge
"BioMed Central will be the most significant development for
disseminating the results of biomedical research in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
World Journal of Surgical Oncology 2008, 6:99 http://www.wjso.com/content/6/1/99
Page 5 of 5
(page number not for citation purposes)
12. Ganz MB, Pachter JA, Barber DL: Multiple receptors coupled to
adenylate cyclase regulate Na-H exchange independent of
cAMP. J Biol Chem 1990, 265:8989-8992.
13. Reubi JC, Laissue J, Krenning E, Lamberts SW: Somatostatin
receptors in human cancer: incidence, characteristics, func-
tional correlates and clinical implications. J Steroid Biochem Mol
Biol 1992, 43:27-35.
14. Daw NC, Billups CA, Rodriguez-Galindo C, McCarville MB, Rao BN,
Cain AM, Jenkins JJ, Neel MD, Meyer WH: Metastatic osteosar-
coma. Cancer 2006, 106:403-412.
15. Meyers PA, Heller G, Healey J, Huvos A, Lane J, Marcove R, Apple-
white A, Vlamis V, Rosen G: Chemotherapy for nonmetastatic
osteogenic sarcoma: the Memorial Sloan-Kettering experi-
ence. J Clin Oncol 1992, 10:5-15.
16. Bacci G, Ferrari S, Mercuri M, Longhi A, Fabbri N, Galletti S, Forni C,
Balladelli A, Serra M, Picci P: Neoadjuvant chemotherapy for
osteosarcoma of the extremities in patients aged 41–60
years: outcome in 34 cases treated with adriamycin, cisplat-
inum and ifosfamide between 1984 and 1999. Acta Orthop
2007, 78:377-384.
17. Alumets J, Sundler F, Hakanson R: Distribution, ontogeny and
ultrastructure of somatostatin immunoreactive cells in the
pancreas and gut. Cell Tissue Res 1977, 185:465-479.
18. Erlandsen SL, Hegre OD, Parsons JA, McEvoy RC, Elde RP: Pancre-
atic islet cell hormones distribution of cell types in the islet
and evidence for the presence of somatostatin and gastrin
within the D cell. J Histochem Cytochem 1976, 24:883-897.
19. Parsons JA, Erlandsen SL, Hegre OD, McEvoy RC, Elde RP: Central
and peripheral localization of somatostatin. Immunoen-
zyme immunocytochemical studies. J Histochem Cytochem 1976,
24:872-882.
20. Srkalovic G, Cai RZ, Schally AV: Evaluation of receptors for
somatostatin in various tumors using different analogs. J Clin
Endocrinol Metab 1990, 70:661-669.
21. Pinski J, Schally AV, Halmos G, Szepeshazi K, Groot K, O'Byrne K, Cai
RZ: Effects of somatostatin analogue RC-160 and bombesin/
gastrin-releasing peptide antagonists on the growth of
human small-cell and non-small-cell lung carcinomas in nude
mice. Br J Cancer 1994, 70:886-892.
22. Enneking WF: A system of staging musculoskeletal neoplasms.
Clin Orthop Relat Res 1986:9-24.
23. Bacci G, Ferrari S, Bertoni F, Ruggieri P, Picci P, Longhi A, Casadei R,
Fabbri N, Forni C, Versari M, Campanacci M: Long-term outcome
for patients with nonmetastatic osteosarcoma of the
extremity treated at the istituto ortopedico rizzoli accord-
ing to the istituto ortopedico rizzoli/osteosarcoma-2 proto-
col: an updated report. J Clin Oncol 2000, 18:4016-4027.
24. Fuchs N, Bielack SS, Epler D, Bieling P, Delling G, Korholz D, Graf N,
Heise U, Jurgens H, Kotz R, et al.: Long-term results of the co-
operative German-Austrian-Swiss osteosarcoma study
group's protocol COSS-86 of intensive multidrug chemo-
therapy and surgery for osteosarcoma of the limbs. Ann Oncol
1998, 9:893-899.
25. Provisor AJ, Ettinger LJ, Nachman JB, Krailo MD, Makley JT, Yunis EJ,
Huvos AG, Betcher DL, Baum ES, Kisker CT, Miser JS: Treatment
of nonmetastatic osteosarcoma of the extremity with pre-
operative and postoperative chemotherapy: a report from
the Children's Cancer Group. J Clin Oncol 1997, 15:76-84.
26. Finkel MP, Reilly CA Jr, Biskis BO: Pathogenesis of radiation and
virus-induced bone tumors. Recent Results Cancer Res
1976:92-103.
27. Swaney JJ: Familial osteogenic sarcoma. Clin Orthop Relat Res
1973:64-68.
28. Guyton AC, Hall JE: Textbook of medical physiology 11th edition. Edin-
burgh: Elsevier Saunders; Oxford: Elsevier Science [distributor]; 2006.
29. Mansky PJ, Liewehr DJ, Steinberg SM, Chrousos GP, Avila NA, Long
L, Bernstein D, Mackall CL, Hawkins DS, Helman LJ: Treatment of
metastatic osteosarcoma with the somatostatin analog
OncoLar: significant reduction of insulin-like growth factor-
1 serum levels. J Pediatr Hematol Oncol 2002, 24:440-446.
30. Ferrari S, Dondi M, Fanti S, Zoboli S, Giacomini S, Mercuri M, Bacci
G: Somatostatin receptor (SSTR) scintigraphy in patients
with osteosarcoma. Cancer Biother Radiopharm 2003, 18:847-851.


























%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)