BioMed Central
Page 1 of 5
(page number not for citation purposes)
World Journal of Surgical Oncology
Open Access
Case report
Giant gluteal lipoma-like liposarcoma: a case report
Maitham Sultan1, Hisham Burezq*1, Rameshwar L Bang2, Moustafa El-
Kabany3 and Waddah Eskaf3
Address: 1Plastic and Reconstructive Surgery, Al-Babtain Center for Burns and Plastic Surgery, Sabah Health area, Ibn-Sina Hospital, PO Box 1574,
Mishref, 40179, State of Kuwait, 2Department of Surgery, Consultant Plastic and Reconstructive Surgeon, Faculty of Medicine, Kuwait University,
State of Kuwait and 3Department of Pathology, Kuwait Cancer Center, Sabah Health Area, State of Kuwait
Email: Maitham Sultan - mkshdt@gmail.com; Hisham Burezq* - burezq@msn.com; Rameshwar L Bang - bangrl@hotmail.com; Moustafa El-
Kabany - moustafawlkabany@hotmail.com; Waddah Eskaf - waddaheskaf@yahoo.com
* Corresponding author
Abstract
Background: Liposarcoma is the second most common soft tissue sarcoma in adults with a peak
incidence between the 4th and 6th decade of life and slight preponderance to the male gender. It
originates from multipotential primitive mesenchymal cells, rather than mature adipose tissue.
Case presentation: An unusual case of a rapidly growing giant lipoma-like liposarcoma of the left
gluteal and perineal areas in a young male was presented. The patient was managed by wide local
excision of the lesion and coverage with split thickness skin graft. The key issues surrounding the
treatment of lipoma-like liposarcoma and literature review is discussed.
Conclusion: For such unusual case of this particular rapidly growing tumor, a longer follow-up is
needed to evaluate the outcome in these cases.
Background
Liposarcoma is the second most common soft tissue sar-
coma in adults. This tumor originates from multipotential
primitive mesenchymal cells rather than mature adipose
tissue [1]. It commonly arises from extremities, particu-
larly thighs, retroperitoneum, inguinal and paratesticular
regions [2,3]. Chest wall, breast, mediastinum, small
intestine, omentum and mesentery may also be involved.
The peak age incidence of well differentiated, dedifferen-
tiated, and pleomorphic liposarcoma occurs between the
4th and 6th decade of life with slight preponderance to the
male gender[1]. The authors described an unusual case of
a rapidly growing giant lipoma-like liposarcoma of the
left gluteal region in a young adult patient. To the best of
our knowledge, no such case is reported in the English lit-
erature.
Case presentation
A 26 year old gentleman presented to our out-patient
clinic at Al-Babtain Center for burns and plastic surgery
with a 16 month history of a rapidly growing mass in the
left gluteal region. Although this mass was interfering sig-
nificantly with his daily normal activities, walking, anal
hygiene and even with defecation, the patient did not
search for treatment until that date when it became
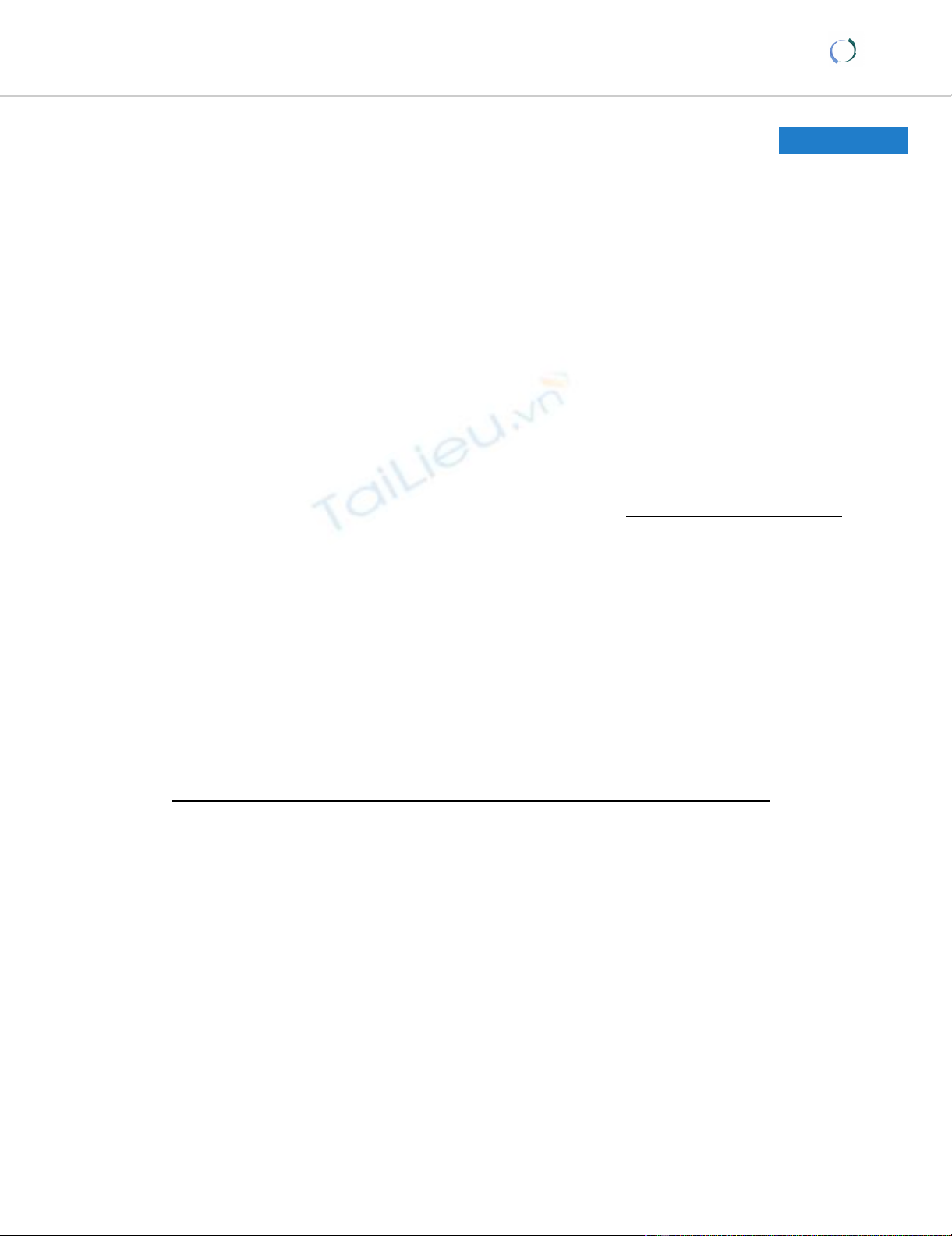
unbearable. Clinical examination revealed a huge well
defined, polypoidal, cutaneous, fleshy mass of about 59
cm × 39 cm × 19 cm occupying most of the left gluteal and
perianal area (Figure 1). The lesion had a narrower pedicle
of about 20 cm × 30 cm. firmly attached to the underlying
subcutaneous tissues. There were areas of peripheral
necrosis associated with multiple patches of ulceration
and foul odor. No pulsations or clinical thrill were identi-
Published: 29 July 2008
World Journal of Surgical Oncology 2008, 6:81 doi:10.1186/1477-7819-6-81
Received: 17 July 2007
Accepted: 29 July 2008
This article is available from: http://www.wjso.com/content/6/1/81
© 2008 Sultan et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Surgical Oncology 2008, 6:81 http://www.wjso.com/content/6/1/81
Page 2 of 5
(page number not for citation purposes)
fied. The systemic clinical examination was within normal
limits. Hematological and biochemical work-up includ-
ing CBC, renal function, liver function and coagulation
profile all showed normal results.
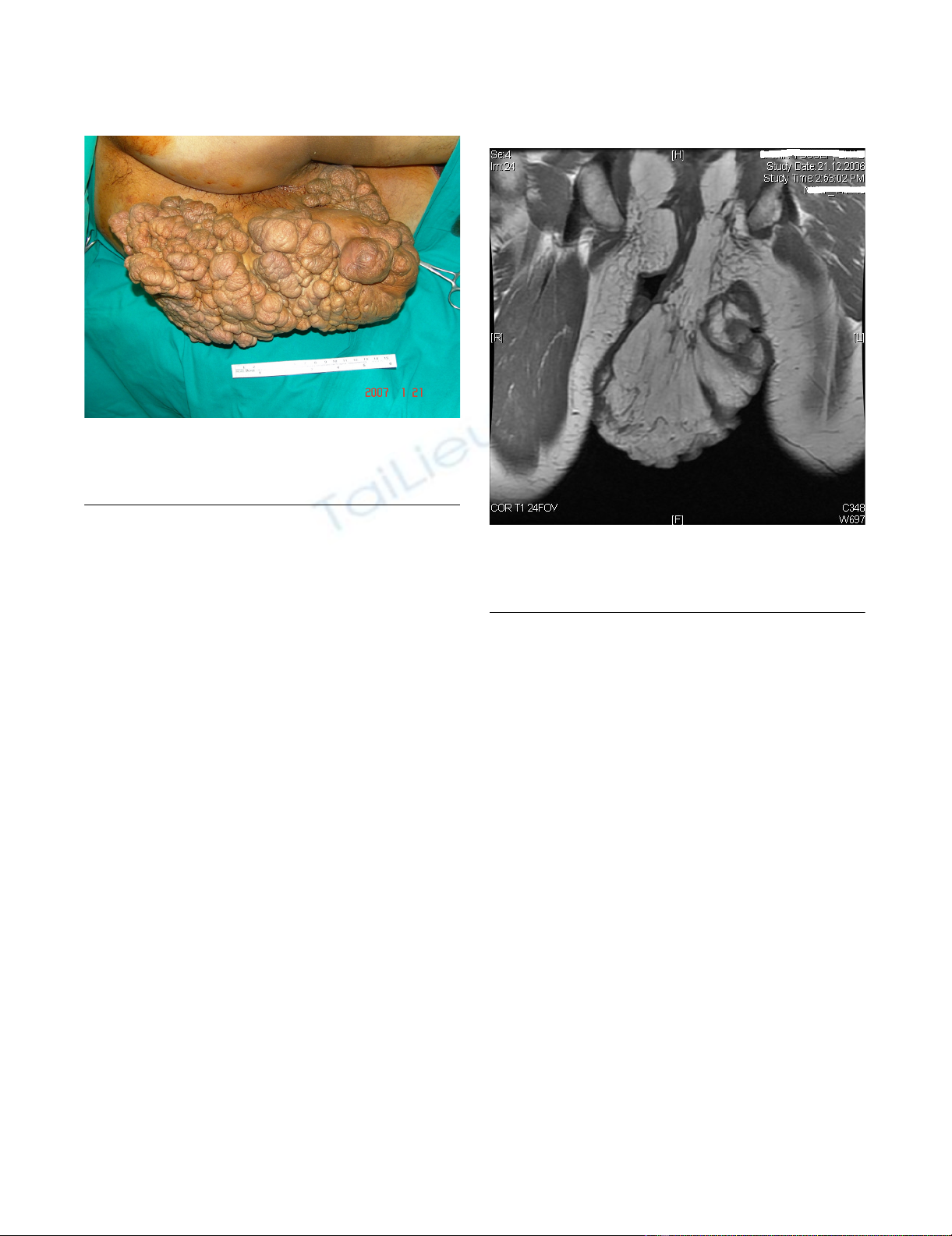
Contrast enhanced MRI showed a huge irregular lobu-
lated mass at the anal region extending outwards and infe-
riorly preserving the anal canal. The mass was mainly of
fatty signal intensity with evidence of solid component
that showed moderate enhancement suggestive of liposa-
rcoma (figure 2). Incisional biopsy was performed to
establish a tissue diagnosis that primarily revealed histo-
logical features of lipofibroma of benign nature. Because
of the huge size and the rapid growth of the lesion and the
possibility of missing the diagnosis with our incisional
biopsy; the decision was taken to completely excise the
lesion with 1 cm free margin down to the sub-fascial plane
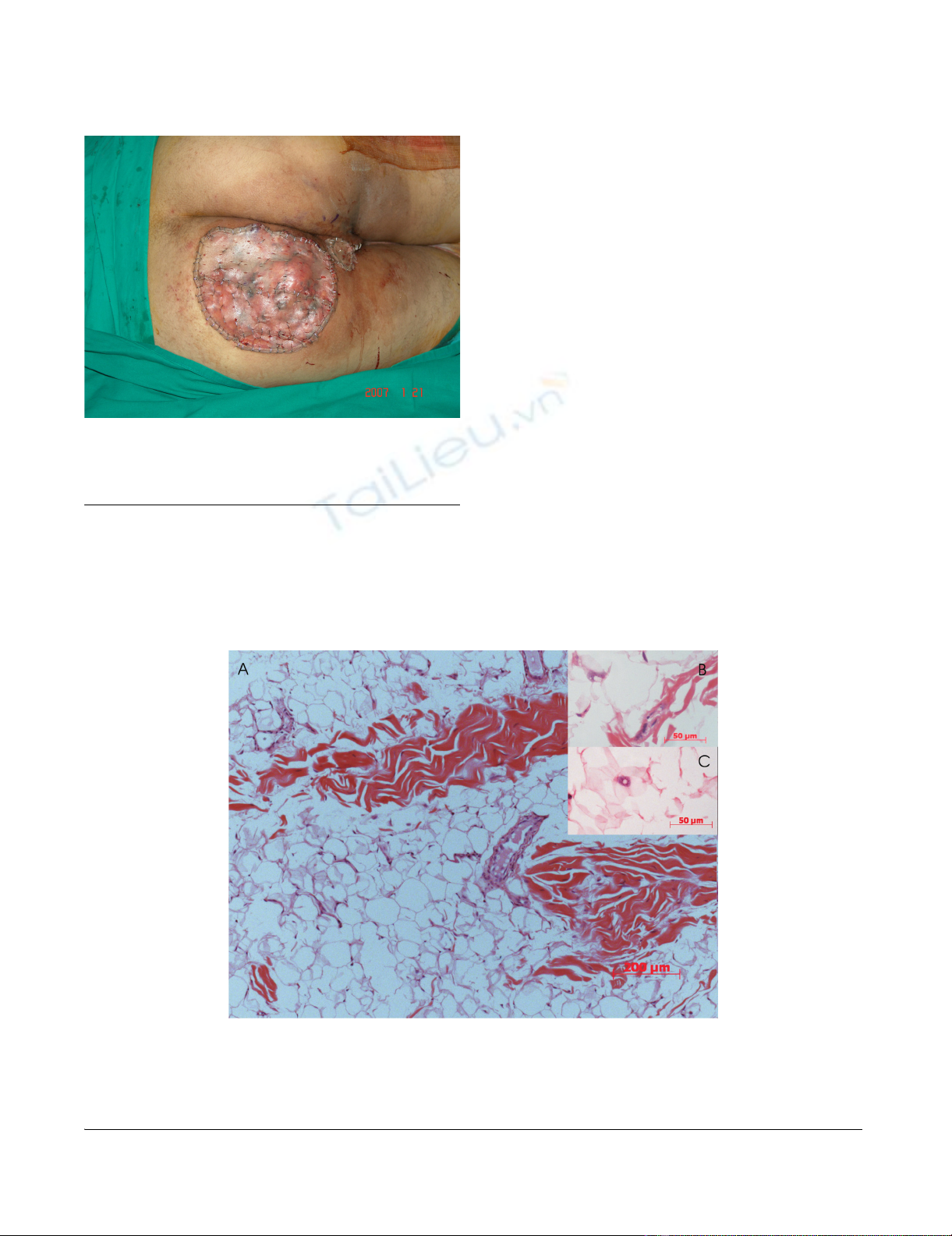
above the gluteal muscles. The excised specimen weighed
2615 grams with subsequent surgical defect about 22 cm
× 27 cm which was reconstructed with a split thickness
skin graft (Figure 3).
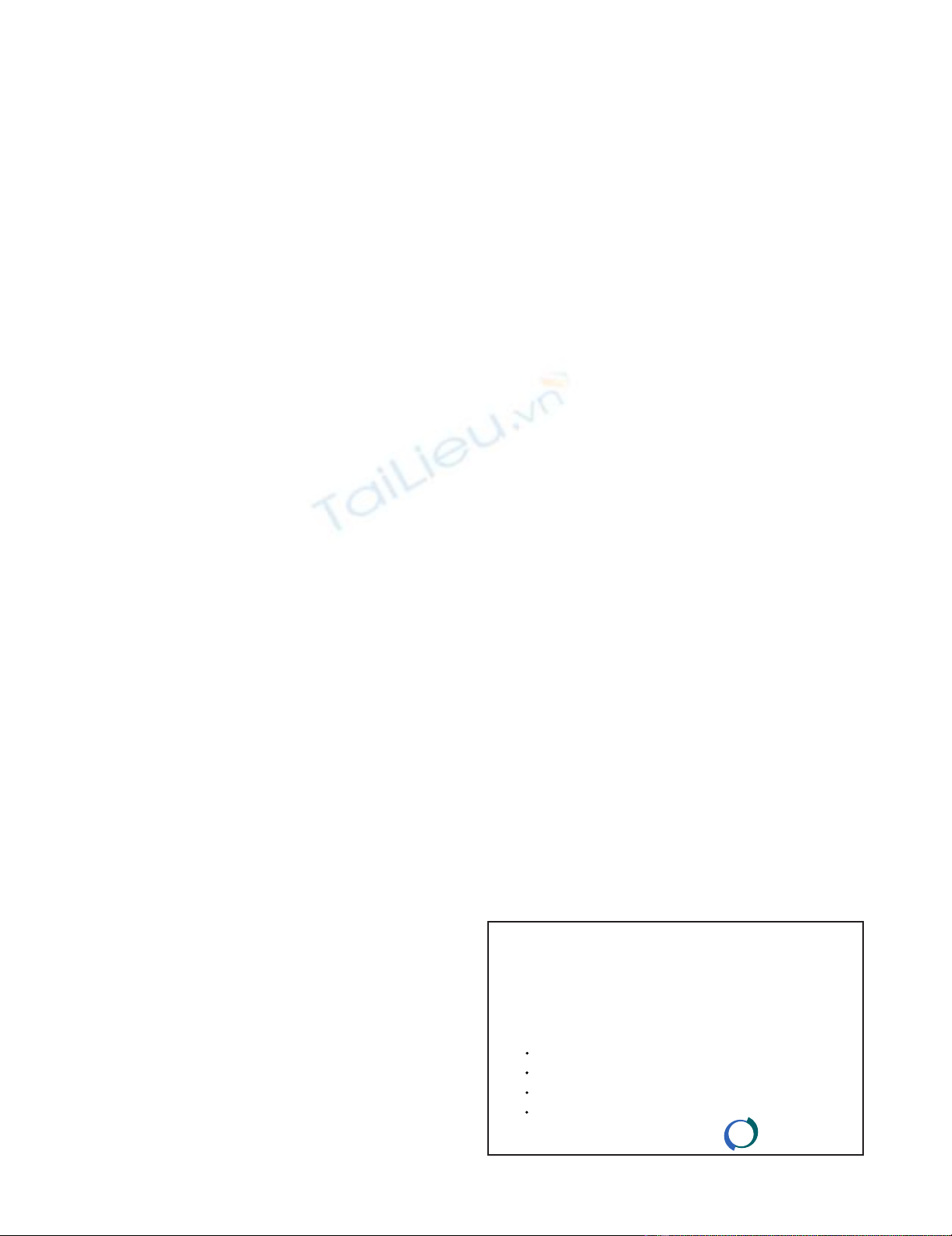
Surprisingly, the final pathology described yellow to
white firm serial section with occasional necrotic foci. His-
tological sections showed variable sized lobules separated
by fibrous septa. The lobules were composed of relatively
mature adipocytic proliferation with significant variation
in cell size, with occasional atypical lipoblasts exhibiting
evidence of nuclear atypia and hyperchromasia. Hyper-
chromatic stromal cells were also, identified in the thick-
ened fibrous bands. Monovacuolated and
multivacuolated lipoblasts as well mononuclear chronic
inflammatory elements were frequently seen (figure 4).
Surface cutaneous tiny ulcerations were noticed and were
partially replaced by inflammatory granulation tissue.
Surgical clearance was adequate.
Post-operative CT scan of the abdomen and pelvis with
oral and IV contrast were done as part of the metastatic
workup and showed no abnormalities.
The case was discussed in the tumor board meeting and
the decision was made to achieve an adequate loco-
regional control by wide local excise. The operation was
done in a left lateral decubitus position under general
anesthesia with oro-tracheal intubation. Total excision of
the lesion was done with a 2 cm free margin down to a
deep sub-facial plane exposing the gluteal maximus mus-
cle which was found to be free of the disease. The resultant
soft tissue defect was covered with a split thickness skin
graft taken from the left thigh. Part of the graft was lost
because of a localized pseudomonas infection which
healed completely with daily wound care and without sur-
gical intervention. The final histopathology diagnosis was
well-differentiated and well defined completely excised
lipoma-like liposarcoma, therefore adjuvant radiotherapy
was not indicated. The patient was followed for about 16
months showing no evidence of recurrence.
T1-MRI axial section showing fatty signal intensity with evi-dence of solid component that showed moderate enhance-ment suggestive of liposarcomaFigure 2
T1-MRI axial section showing fatty signal intensity
with evidence of solid component that showed mod-
erate enhancement suggestive of liposarcoma.
Intra-operative photo showing a large polypoidal mass involv-ing most of the left gluteal and perianal areaFigure 1
Intra-operative photo showing a large polypoidal
mass involving most of the left gluteal and perianal
area.
World Journal of Surgical Oncology 2008, 6:81 http://www.wjso.com/content/6/1/81
Page 3 of 5
(page number not for citation purposes)
Discussion
Adipocytic tumors represent the largest single group of
mesenchymal neoplasms, due to the high prevalence of
lipomas and their variants. Liposarcoma represents the
single most common soft tissue sarcoma in adults,
accounting for approximately 20% of all cases[4]. Its prin-
cipal histological subtypes; well differentiated, myxoid/
round cell and pleomorphic are entirely separate diseases
with different morphology, genetics and natural history.
The principal changes in the recent WHO classification
demonstrates that atypical lipomatous tumors and well
differentiated liposarcoma are essentially synonymous
and that site-specific variations in behavior relate only to
surgical resectability [5].
This male patient was quite young though the peak inci-
dence is considered between the 4th and 6th decade of
life[1]. The presentation was due to the discomfort in
maintaining the day today activities and foul odor it emit-
ted. The lesion was a cutaneous outward growth and it
attained considerable size in a short period of time and
presented a difficult dilemma for the diagnosis.
Liposarcomas can be divided into three basic histological
categories; well-differentiated liposarcomas which mor-
phologically subdivided into lipoma-like, sclerosing,
inflammatory or spindle cell type, myxoid liposarcoma
and pleomorphic liposarcoma [5].
Well-differentiated liposarcomas account for about 40%–
45% of all liposarcoma and therefore represent the larger
subgroup of adipocytic malignancies. Although the recur-
Intra-operative photo showing the defect created after total resection and split thickness meshed skin graftingFigure 3
Intra-operative photo showing the defect created
after total resection and split thickness meshed skin
grafting.
Photomicrograph of excised lesion showing a well differentiated lipomatous tumor growth which exhibits at low magnification adipocyte with significant variation in size and shape (A) as well as occasional atypical adipocyte with enlarged hyperchromatic nuclei seen with high magnification (arrow)(B & C) (H&E stained, 5 u thick paraffin sections)Figure 4
Photomicrograph of excised lesion showing a well differentiated lipomatous tumor growth which exhibits at
low magnification adipocyte with significant variation in size and shape (A) as well as occasional atypical adi-
pocyte with enlarged hyperchromatic nuclei seen with high magnification (arrow)(B & C) (H&E stained, 5 u
thick paraffin sections).

World Journal of Surgical Oncology 2008, 6:81 http://www.wjso.com/content/6/1/81
Page 4 of 5
(page number not for citation purposes)
rence rate can reach up to 30% of the cases, this tumor
which is surgically amenable behaves as a benign neo-
plasm and is not known to metastasize, thus requiring a
less aggressive treatment [6]. The most important prog-
nostic factor for well-differentiated liposarcoma is its ana-
tomic location where superficial lesions are considered
favorable while deeply seated lesions such as retroperito-
neal or mediastinal liposarcoma are associated with
increased recurrence and metastatic rates [1,6].
The benefit of wide local excision over marginal excision
is recognized in the literature [7]. In our case, we have
excised the lesion with 1 cm margin down to a subfascial
plane over the gluteal muscles to have good local control.
We could not find any evidence in the literature suggest-
ing a benefit in outcome with the use of postoperative
radiotherapy. Some authors caution against its use to treat
this lesion due to the uncertainty about its role in the ded-
ifferentiation process 4.
Conclusion
An unusual case of a rapidly growing, giant gluteal
lipoma-like liposarcoma was presented. Surgical excision
is the main treatment for most primary soft tissue sarco-
mas. As such every effort should be made to achieve com-
plete tumor resection. A longer follow-up is needed to
evaluate the outcome such cases. Although not used in
this case, we wonder if radiotherapy could be used in such
giant tumors to improve the loco-regional control.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
HB Substantial contributions to conception, design, and
in drafting the manuscript or revising it critically for
important intellectual content. MS Substantial contribu-
tion in literature review and data analysis. RLB Substantial
contributions in reviewing the draft and the addition of
important data to the text. WE analysis of slides taken
from the patient and reaching a diagnosis. ME analyzed
the data related to pathology in the text with a significant
contribution in drafting. All authors read and approved
the final manuscript.
Acknowledgements
The reporting of this case was approved by the ethics committee of Al-
Babtain center for Burns and plastic surgery, Ibn-Sina Hospital, Sabah
Health Centre, State of Kuwait.
References
1. Amato G, Martella A, Ferraraccio F, Di Martino N, Maffettone V, Lan-
dolfi V, Fei L, Del Genio A: Well differentiated "lipoma-like"
liposarcoma of the sigmoid mesocolon and multiple lipoma-
tosis of the rectosigmoid colon. Report of a case. Hepatogas-
troenterology 1998, 45(24):2151-2156.
2. Montgomery E, Fisher C: Paratesticular liposarcoma: a clinico-
pathologic study. Am J Surg Pathol 2003, 27(1):40-47.
3. Dalla Palma P, Barbazza R: Well-differentiated liposarcoma of
the paratesticular area: report of a case with fine-needle
aspiration preoperative diagnosis and review of the litera-
ture. Diagn Cytopathol 1990, 6(6):421-426.
4. Sommerville SM, Patton JT, Luscombe JC, Mangham DC, Grimer RJ:
Clinical outcomes of deep atypical lipomas (well-differenti-
ated lipoma-like liposarcomas) of the extremities. ANZ J Surg
2005, 75(9):803-806.
5. Dei Tos AP: Liposarcoma: new entities and evolving concepts.
Ann Diagn Pathol 2000, 4(4):252-266.
6. Laurino L, Furlanetto A, Orvieto E, Del Tos AP: Well-differenti-
ated liposarcoma (atypical lipomatous tumors). Semin Diagn
Pathol 2001, 18(4):258-262.
7. Capodiferro S, Scully C, Maiorano E, Lo Muzio L, Favia G: Liposar-
coma circumscriptum (lipoma-like) of the tongue: report of
a case. Oral Dis 2004, 10(6):398-400.
Publish with BioMed Central and every
scientist can read your work free of charge
"BioMed Central will be the most significant development for
disseminating the results of biomedical researc h in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
World Journal of Surgical Oncology 2008, 6:81 http://www.wjso.com/content/6/1/81
Page 5 of 5
(page number not for citation purposes)


























%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)