BioMed Central
Page 1 of 4
(page number not for citation purposes)
World Journal of Surgical Oncology
Open Access
Case report
Isolated metastatic extremity liposarcoma to the liver, an
uncommon and transient finding
Christopher A Garces1, John D Reith2, Stephen R Grobmyer1 and
Steven N Hochwald*1
Address: 1Division of Surgical Oncology, Department of Surgery, University of Florida, Box 100286, Gainesville, Florida, 32610, USA and
2Departments of Pathology, Immunology and Laboratory Medicine, University of Florida, Box 100275, Gainesville, Florida, 32610, USA
Email: Christopher A Garces - christopher.garces@surgery.ufl.edu; John D Reith - reith@pathology.ufl.edu;
Stephen R Grobmyer - stephen.grobmyer@surgery.ufl.edu; Steven N Hochwald* - hochwsn@surgery.ufl.edu
* Corresponding author
Abstract
Background: Extremity liposarcomas can metastasize to different areas of the body but have
rarely been demonstrated to metastasize to the liver. Due to the unusual occurrence of isolated
metastatic extremity liposarcoma to the liver, the optimal treatment of this condition is unknown.
Case presentation: Less than one year after resection of a myxoid/round cell liposarcoma of the
left lateral calf, a 61-year-old male presented with a CT scan showing a 2 cm low-density lesion in
the right lobe of the liver. The lesion tripled in size over the next few months. An extensive
evaluation revealed isolated disease to the liver. The lesion was surgically removed with a right
hepatic lobectomy and the pathology was consistent with metastatic myxoid/round cell
liposarcoma.
Conclusion: Although extremity liposarcoma rarely metastasizes solely to the liver, the best
chance at cure is with complete resection. Unfortunately, cure rates are very low in the setting of
metastatic disease. As expected, the patient experienced progression of disease at sites outside of
the liver 5 months after the liver resection.
Background
Extremity soft tissue sarcomas are rare mesenchymal
tumors with 3,900 new cases being diagnosed each year
and are typically malignant fibrohistiocytoma, liposar-
coma, or synovial sarcomas. Myxoid liposarcomas make
up 38% of liposarcomas with round cell tumors (11%)
and mixed lesions (8%) less commonly present [1,2].
Prognostic factors that impact on survival include histo-
logical grade and size [3]. The histological subtype of the
liposarcoma and extent of round cell component is
thought to be an important determinant of outcome. The
incidence of metastatic disease is 29–33% for myxoid,
13% for round cell, and 40% for mixed [2,4,5].
Management of metastatic disease is a difficult problem
with no clear consensus. Chemotherapy has had limited
results outside of case reports [6,7]. The most common
patterns of metastasis for myxoid liposarcomas are to the
lung and retroperitoneum [2,6].
Published: 9 October 2008
World Journal of Surgical Oncology 2008, 6:108 doi:10.1186/1477-7819-6-108
Received: 20 June 2008
Accepted: 9 October 2008
This article is available from: http://www.wjso.com/content/6/1/108
© 2008 Garces et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Surgical Oncology 2008, 6:108 http://www.wjso.com/content/6/1/108
Page 2 of 4
(page number not for citation purposes)
Hepatic metastases from a primary extremity soft-tissue
sarcoma are rare [6]. There is one case report demonstrat-
ing the liver as the first site of spread from an extremity
myxoid liposarcoma [7]. There is little information
regarding the appropriate management of these lesions.
We report an unusual case of a mixed myxoid/round cell
liposarcoma of the extremity with an isolated hepatic
metastasis, treated by liver resection. Although disease in
the liver was determined to be the only site of disease
upon initial tumor recurrence, the patient experienced
progression of disease outside of the liver 5 months after
the liver directed therapy.
Case presentation
A 61-year-old male noted a mass in his left lateral calf. A
biopsy was performed revealing a myxoid liposarcoma.
The patient subsequently underwent resection of an 8.0 ×
6.0 × 3.5 cm tumor with wide margins (Figure 1). Histo-
logically, greater than 95% of the mass consisted of
myxoid liposarcoma with extensive hypercellular ("transi-
tional") foci (Figure 2), and less than 5% consisted of
round cell liposarcoma (Figure 3). The tumor was classi-
fied as grade 2 of 3.
The patient did well for 14 months, but follow-up com-
puted tomography (CT) demonstrated an asymptomatic
6.3 by 6.8 cm mass in the right lobe of the liver that was
growing in size (Figure 4). A PET/CT scan was done that
showed the liver lesion was not FDG avid and there was
no other metastatic disease. Due to concern of isolated
metastatic disease to the liver, resection was recom-
mended.
At laparotomy, ultrasound showed a large mass present in
the right lobe of the liver and that the mass splayed the
anterior and posterior portal pedicles apart. Next, a stand-
ard right hepatic lobectomy was performed with negative
margins (Figure 5). A 7.3 × 6.5 × 7.0 cm mass of metastatic
myxoid/round cell liposarcoma was present in the liver
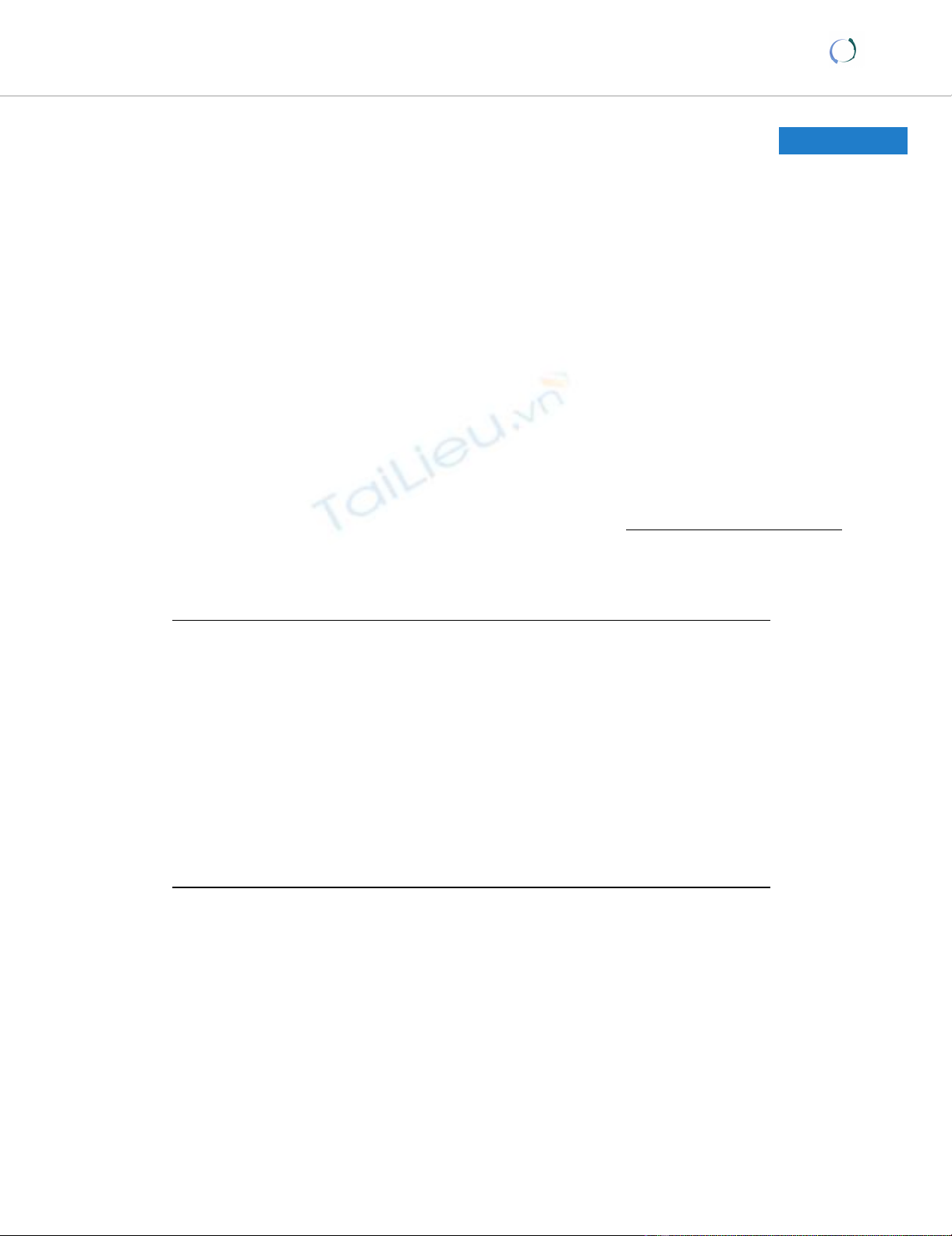
Gross pathologic photograph of the primary tumor resected from the legFigure 1
Gross pathologic photograph of the primary tumor
resected from the leg. The tumor has a significant fat
component and is relatively well circumscribed.
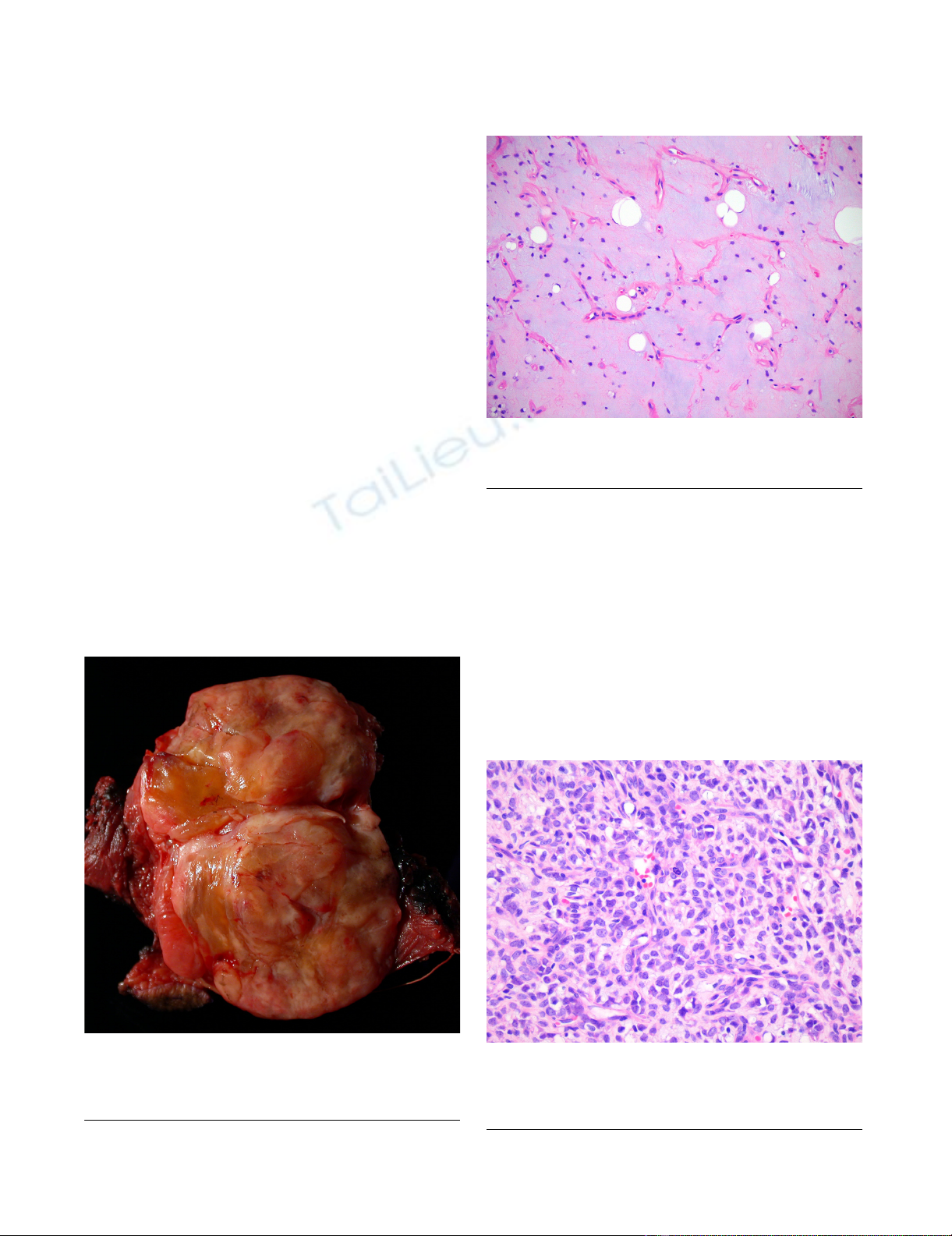
Histologic section of the primary tumor in the extremity showing a liposarcomaFigure 2
Histologic section of the primary tumor in the
extremity showing a liposarcoma.
Histologic section of the primary tumor in the extremity showing a round cell component comprising < 5% of the tumorFigure 3
Histologic section of the primary tumor in the
extremity showing a round cell component compris-
ing < 5% of the tumor.
World Journal of Surgical Oncology 2008, 6:108 http://www.wjso.com/content/6/1/108
Page 3 of 4
(page number not for citation purposes)
with histologic features virtually identical to those seen in
the calf mass (Figure 6). The patient had an uneventful
post-operative course.
Five months after the resection of the isolated liver metas-
tases the patient was found to have a metastatic lesion on
the chest wall and spinal metastases. The patient suc-
cumbed to disease during follow-up.
Discussion
Liposarcomas consists of five subtypes: well differenti-
ated, myxoid, round cell, pleomorphic, and mixed. The
myxoid subtype is the most common variant of extremity
liposarcomas and has a high predilection to extrapulmo-
nary sites of metastasis. The most common being the ret-
roperitoneum. A mixed myxoid/round cell component as
seen in this case is found in 8% of patients presenting with
an extremity liposarcoma [2]. Investigators at the Royal
Marsden Hospital in London evaluated 50 patients with
myxoid liposarcomas with a median follow-up of 43
months. They concluded that any round cell component
of the myxoid liposarcoma was associated with a greater
chance of metastatic disease [5].
The most common site of spread is to the lung from
extremity sarcomas and the incidence is dependent on
tumor grade and size. Hepatic metastases from primary
soft tissue sarcomas (STS) frequently occur in cases of vis-
ceral and retroperitoneal tumors. It is uncommon for
extremity soft-tissue sarcomas to spread to the liver (<
0.5%) [6]. It is even rarer for the tumor metastasis to be
isolated to the liver, such as this case. The group at Memo-
rial Sloan Kettering Cancer Center identified 637 patients
with extremity soft tissue sarcomas and never was the liver
the first or sole site for metastasis [6]. Similar results were
seen at Massachusetts General Hospital. Twenty-two
patients were identified with extra-pulmonary metastatic
extremity myxoid liposarcoma and none of them pre-
sented with isolated liver metastases [2]. There are other
case reports of extremity liposarcoma solely metastasizing
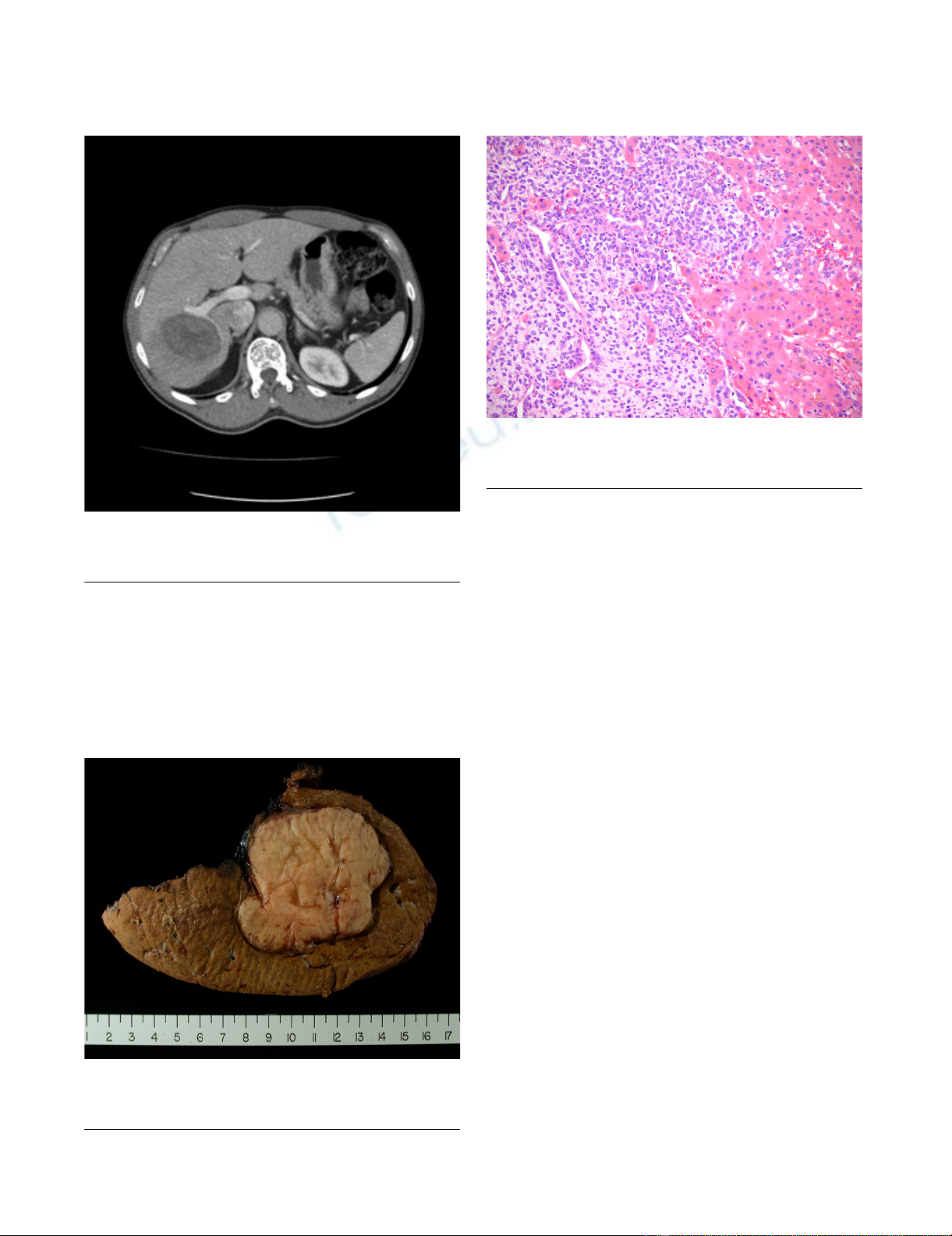
Triple-phase abdominal CT showing 7 cm low-density lesion in right lobe of liverFigure 4
Triple-phase abdominal CT showing 7 cm low-den-
sity lesion in right lobe of liver.
Liver resection specimen showing well circumscribed tumor with fat componentFigure 5
Liver resection specimen showing well circumscribed
tumor with fat component.
Histologic section of the metastatic disease in the liver show-ing extensive round cell componentFigure 6
Histologic section of the metastatic disease in the
liver showing extensive round cell component.

World Journal of Surgical Oncology 2008, 6:108 http://www.wjso.com/content/6/1/108
Page 4 of 4
(page number not for citation purposes)
to the heart, pancreas, larynx, thyroid gland, and brain [8-
14]. There is only one case in the literature of an extremity
myxoid liposarcoma with isolated distant metastasis to
the liver [7].
There are few treatment options for metastatic soft tissue
sarcomas (STS) to the liver. Conventional chemotherapy
has not impacted survival in patients with metastatic STS
to the liver. The group at MSKCC treated 52 of 65 patients
with STS with hepatic metastases with a doxorubicin-
based chemotherapy and the partial response rate was 6%
with no complete responders [6]. Each patient was con-
sidered for hepatic resection, but only 14 patients were
resectable. Free margins were achieved in 13/14 patients.
All the patients had recurrence in the liver but median sur-
vival was 30 months in the resected group compared to 12
months in the unresected group. In this study only 4/14
resected patients had an extremity STS as their primary
tumor. In addition, there were no 5-year survivors. The
overall 5-year survival for pooled data of 48 patients with
STS metastatic to liver who underwent hepatic resections
was 11% [6].
There is a single case report of a patient with an isolated
hepatic metastasis from an extremity liposarcoma who
underwent resection and remained alive for 22 years [7].
This patient underwent numerous regimens for distant
recurrences over the years. The regimens included doxoru-
bicin, ifosfamide, and etoposide. The patient had stabili-
zation of disease, but never cures of it.
Complete resection of liver disease is the only means for
long-term survival in metastatic extremity liposarcoma
but cure is rarely achieved. Unfortunately, the patient in
this case report had a short disease free interval following
liver resection and was identified to have disease on the
chest wall and spine after 5 months. Consideration
should be given for "adjuvant" therapy following resec-
tion of metastatic sarcoma. However, the most active
chemotherapeutic options for sarcoma are of limited
value and are associated with serious and potentially life-
threatening toxicity. Median survival from the time metas-
tases are recognized is on the order of 12 months,
although 20% to 25% of patients with metastatic sarcoma
are alive 2 years after diagnosis. In fact, the most recent
study which was the largest undertaken of adjuvant chem-
otherapy in soft tissue sarcoma failed to demonstrate a
survival benefit [15].
Conclusion
Optimal treatment of patients with unresectable or meta-
static soft tissue sarcoma requires an understanding of the
natural history of the disease, close attention to the indi-
vidual patient and an understanding of the benefits and
limitations of the therapeutic options.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
CAG assembled data and participated in drafting of the
manuscript. JDR assembled data and reviewed pathology.
SRG participated in writing the manuscript and critical
review. SNH conceived concept, assembled data, partici-
pated in drafting of the manuscript and critical review.
Consent
Patient consent could not be obtained as the patient died,
the case was presented to the Health centre Institutional
Review Board of University of Florida and an IRB exemp-
tion was obtained.
References
1. Clarkson P, Ferguson PC: Primary multidisciplinary manage-
ment of extremity soft tissue sarcomas. Curr Treat Options
Oncol 2004, 5:451-462.
2. Estourgie SH, Nielsen GP, Ott MJ: Metastatic patterns of
extremity myxoid liposarcoma and their outcome. J Surg
Oncol 2002, 80:89-93.
3. Grobmyer SR, Brennan MF: Predictive variables detailing the
recurrence rate of soft tissue sarcomas. Curr Opin Oncol 2003,
15:319-326.
4. Pearlstone DB, Pisters PW, Bold RJ, Feig BW, Hunt KK, Yasko AW,
Patel S, Pollack A, Benjamin RS, Pollock RE: Patterns of recurrence
in extremity liposarcoma: implications for staging and fol-
low-up. Cancer 1999, 85:85-92.
5. Spillane AJ, Fisher C, Thomas JM: Myxoid liposarcoma – the fre-
quency and the natural history of nonpulmonary soft tissue
metastases. Ann Surg Oncol 1999, 6:389-394.
6. Jaques DP, Coit DG, Casper ES, Brennan MF: Hepatic metastases
from soft-tissue sarcoma. Ann Surg 1995, 221:392-397.
7. Merimsky O, Terrier P, Stanca A, Le CT, Spielmann M, Tursz T, Le
CA: Liver metastases from extremity soft tissue sarcoma.
Am J Clin Oncol 1999, 22:70-72.
8. Bailey SC, Bailey B, Smith NT, Van TP, Thomas CR Jr: Brain metas-
tasis from a primary liposarcoma of the digit: case report.
Am J Clin Oncol 2001, 24:81-84.
9. Carboni F, Ettorre GM, Lorusso R, Lepiane P, Santoro R, Mancini P,
Di Matteo FM, Santoro E: Isolated pancreatic metastasis of
extremity myxoid liposarcoma: Report of a case. Jpn J Clin
Oncol 2006, 36:662-664.
10. Chughtai A, Cronin P, Lucas DR, Prager R, Kazerooni EA: Meta-
static shoulder liposarcoma to the right ventricle: CT find-
ings. J Thorac Imaging 2007, 22:195-198.
11. Daly SF, Sciubba J, Tufano RP: Lower-extremity liposarcoma
metastatic to the larynx: case report. Ear Nose Throat J 2006,
85:185-6, 189.
12. Haft H, Wang GC: Metastatic liposarcoma of the brain with
response to chemotherapy: case report. Neurosurgery 1988,
23:777-780.
13. Sugiyama K, Okubo T, Kamigaki Y, Kin H: Cardiac metastatic
liposarcoma. Jpn J Thorac Cardiovasc Surg 2000, 48:663-665.
14. Tysome JR, Sandison A, Clarke PM: Myxoid liposarcoma meta-
static to the thyroid gland: a case report and literature
review. J Laryngol Otol 2006, 120:511-513.
15. Woll PJ, van Glabbeke M, Hohenberger A, Le Cesne A, Gronchi A,
Hoekstra HJ, Radford JA, van Coevorden F, Blay J: Adjuvant Chem-
otherapy (CT) with Doxorubicin and Ifosfamide in Resected
Soft Tissue Sarcoma (STS): Interim Analysis of a Ran-
domised Phase III Trial. Journal of Clinical Oncology 2007,
25:10008.


























%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)