BioMed Central
Page 1 of 5
(page number not for citation purposes)
World Journal of Surgical Oncology
Open Access
Technical innovations
Major liver resection for hepatocellular carcinoma in the morbidly
obese: A proposed strategy to improve outcome
Omar Barakat*1, Mark D Skolkin2, Barry D Toombs2, John H Fischer II2,
Claire F Ozaki1 and R Patrick Wood1
Address: 1Department of Surgery, the Texas Heart Institute at St. Luke's Episcopal Hospital, Houston, Texas, USA and 2Department of
Interventional Radiology, The Texas Heart Institute at St. Luke's Episcopal Hospital, Houston, Texas, USA
Email: Omar Barakat* - omarbarakat@sbcglobal.net; Mark D Skolkin - mskolkin@sleh.com; Barry D Toombs - btoombs@sleh.com;
John H Fischer - jfischer@sleh.com; Claire F Ozaki - c0z@flash.net; R Patrick Wood - rpwood7070@sbcglobal.net
* Corresponding author
Abstract
Background: Morbid obesity strongly predicts morbidity and mortality in surgical patients.
However, obesity's impact on outcome after major liver resection is unknown.
Case presentation: We describe the management of a large hepatocellular carcinoma in a
morbidly obese patient (body mass index >50 kg/m2). Additionally, we propose a strategy for
reducing postoperative complications and improving outcome after major liver resection.
Conclusion: To our knowledge, this is the first report of major liver resection in a morbidly obese
patient with hepatocellular carcinoma. The approach we used could make this operation nearly as
safe in obese patients as it is in their normal-weight counterparts.
Background
Obesity is perhaps the most significant public health
problem facing the United States and the Western world
today. Each year, an estimated 300,000 Americans die
from obesity-related illnesses [1]. The latest National
Health and Nutrition Examination data show that the
prevalence of obesity with body mass index (BMI) ≥ 30
kg/m2 has increased from 22.9% in 1994 to 30.5% in
2000. The prevalence of morbid obesity (BMI ≥ 40 kg/m2)
also significantly increased, from 2.9% to 4.7% [2]. This
increase has affected most surgical practices, as surgeons
are operating on obese patients in increasing numbers
[3,4].
Perioperative morbidity, mortality, and prolonged hospi-
tal stays are particularly common in obese patients,
because these patients often have preexisting cardiac and
respiratory disease [3,5]. Moreover, epidemiologic studies
have shown that obesity and diabetes are frequently asso-
ciated with nonalcoholic fatty liver disease, which
includes a spectrum of liver disorders that may progress to
hepatocellular carcinoma (HCC) [6,7]. Although several
studies have analyzed the impact of obesity on patients
after major surgical procedures, including liver transplan-
tation [4,8,9], there are, to our knowledge, no data on the
outcome of major liver resection for HCC in morbidly
obese patients.
Published: 10 September 2008
World Journal of Surgical Oncology 2008, 6:100 doi:10.1186/1477-7819-6-100
Received: 20 May 2008
Accepted: 10 September 2008
This article is available from: http://www.wjso.com/content/6/1/100
© 2008 Barakat et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Surgical Oncology 2008, 6:100 http://www.wjso.com/content/6/1/100
Page 2 of 5
(page number not for citation purposes)
In this report, we discuss the treatment of a large HCC in
a morbidly obese patient with a BMI greater than 50 kg/
m2. We also discuss the current literature on surgical com-
plications in obese patients, and we make some general
recommendations about treating HCC in such patients.
Case presentation
A 41-year-old woman presented with a 2-month history
of pruritus. Her medical history included morbid obesity
(BMI, 56 kg/m2), hypertension, and type II diabetes. Her
initial liver function tests showed moderately elevated
total bilirubin and alkaline phosphatase levels and a nor-
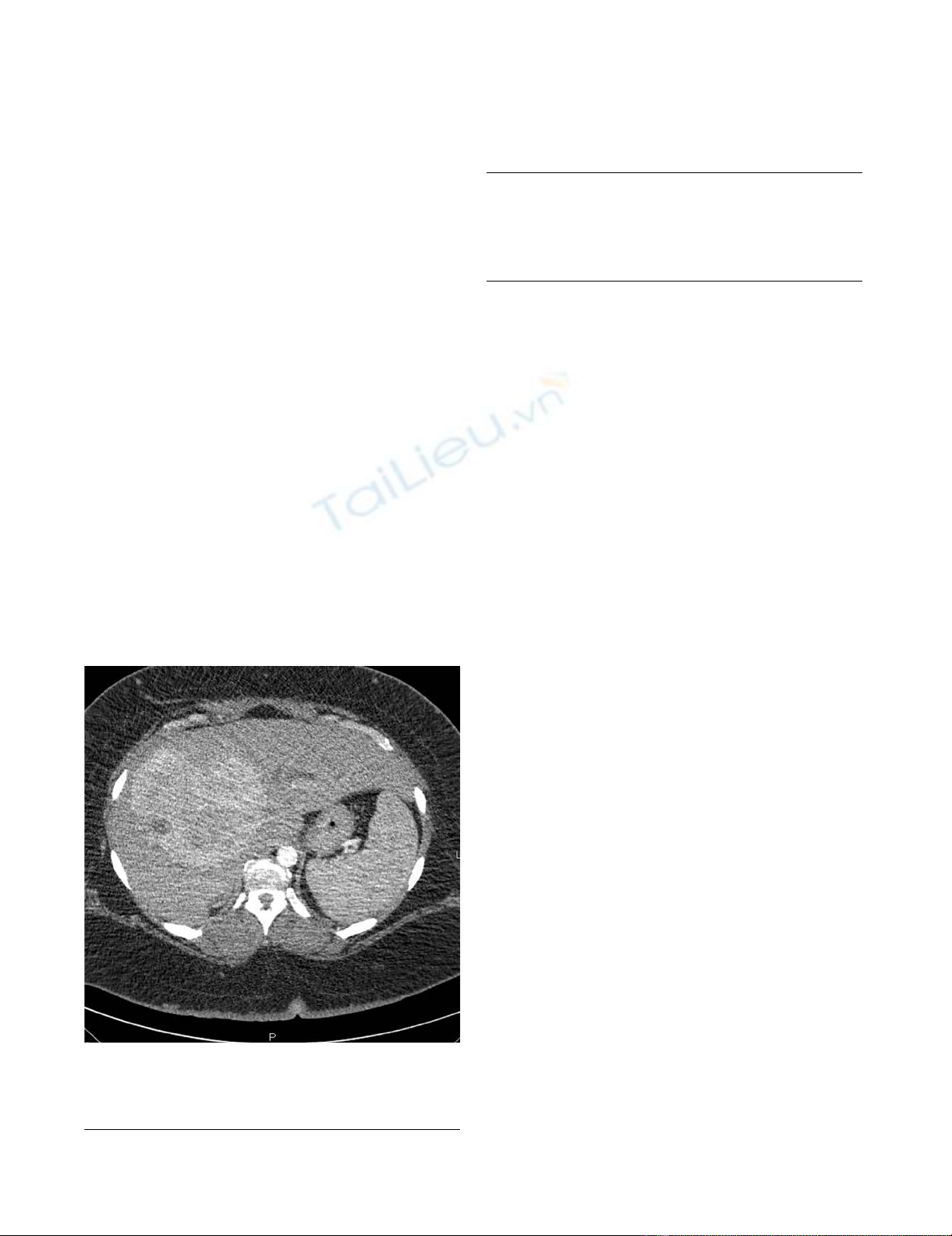
mal alpha-fetoprotein (AFP) level (Table 1). A computed
tomography scan (CT-scan) revealed a large (14-cm),
hypervascular mass that involved segment IV of the left
lobe and segments V and VIII of the right lobe of the liver,
partially occluding the proximal part of the common bile
duct and causing moderate dilatation of the intrahepatic
biliary system (Figure 1). Percutaneous biopsy of the
tumor confirmed well-differentiated HCC. In addition,
biopsy of segment II of the left lobe revealed mild hepati-
tis with no evidence of steatosis. Volumetric measurement
showed that segments I, II, and III accounted for less than
20% of the total liver volume and less than 0.45% of the
patient's total body weight.
Surgical resection was initially ruled out because of a
small-for-size remnant liver and abnormal pulmonary
function tests that suggested a combination of restrictive
and peripheral airway diseases (Table 2). After discussing
with the patient the risk of complications and potential
liver failure associated with extensive liver resection, we
elected to pursue locoregional therapy consisting of
hepatic transarterial chemo/radioembolization with dox-
orubicin and yttrium-90 (Y-90) microspheres (Sirtex
Medical Limited, Lake Forest, IL, USA). The patient was
also placed on a weight-reduction program based on a
hypocaloric Mediterranean diet, which has been proven
effective for weight loss. Protein intake was calculated as 1
g/kg of body weight. The patient was also instructed to
enroll in an aerobic and resistance exercise program in an
attempt to improve her metabolic syndrome.
The treatment protocol consisted of 6 weekly injections of
doxorubicin mixed with ethiodized oil, followed by 500-
to 700-micron Embospheres (Biosphere Medical Inc,
Rockland, MA, USA) alternated with Y-90 microspheres
injected selectively into the right and middle hepatic arter-
ies by interventional radiologists. The patient underwent
5 cycles of treatment; side effects were minimal and were
related to postembolization effects. The total cumulative
doses of doxorubicin and Y-90 were 200 mg and 40.4
mCi, respectively.
After 7 months of treatment, a follow-up CT scan of the
abdomen showed no significant change in the size and
enhancement pattern of the tumor. However, the patient's
weight had decreased from 159 kg to 136 kg (so that BMI
decreased from 56 to 48 kg/m2). This change was accom-
panied by improvements in most pulmonary function
parameters (Table 2) and reductions in the dosage of the
patient's antihypertensive and antidiabetic medications.
At that time, the decision was made to proceed with
extended right hepatectomy to remove segments IV, V, VI,
VII, and VIII after right portal vein embolization (PVE) to
allow compensatory hypertrophy of segments II and III. A
volumetric study performed 8 weeks after PVE showed
that the caudate lobe and segments II and III accounted
for 33% of the total liver volume.
Surgical technique
The patient underwent an extended right hepatectomy.
She was positioned on a bariatric operating table (Maquet
surgical table; Getinge AB, Getinge, Sweden). Exploratory
A triple-phase helical CT scan shows a 14-cm hypervascular mass involving the right lobe and the medial segment of the left lobe of the liverFigure 1
A triple-phase helical CT scan shows a 14-cm hyper-
vascular mass involving the right lobe and the medial
segment of the left lobe of the liver.
Table 1: Preoperative liver function tests and alpha-fetoprotein
(AFP) level
Total bilirubin (mg/dL) 1.8
Alkaline phosphatase (IU/L) 280
Alanine aminotransferase, ALT (IU/L) 80
Aspartate aminotransferase, AST (IU/L) 81
Albumin (g/dL) 3.8
AFP (ng/mL) 3
World Journal of Surgical Oncology 2008, 6:100 http://www.wjso.com/content/6/1/100
Page 3 of 5
(page number not for citation purposes)
laparotomy was performed through bilateral subcostal
incisions with upper midline extensions. A bariatric
Thompson self-retaining retractor (Thompson Surgical
Instruments, Inc., Traverse City, MI, USA) was used to ele-
vate the costal margins and facilitate exposure. Despite
extensive locoregional therapy, there was minimal inflam-
matory reaction and adhesions between the liver and
adjacent organs. Intraoperative ultrasound was used to
confirm the previously defined anatomic relation of the
tumor with the intrahepatic vasculature. Hilar dissection
and mobilization of the right lobe of the liver were carried
out in standard fashion for extended right hepatectomy.
Parenchymal transaction was performed with a dissecting
sealer (TissueLink Medical, Inc., Dover, NH, USA). The
total operative time was 630 min. Estimated blood loss
was 720 mL. No transfusion of blood products was
required.
The patient's postoperative course was uneventful, despite
the long operative time and the technical difficulties
encountered during mobilization of the liver because of
the compensatory hypertrophy of the left lateral segment
and the tumor's large size. The patient remained in the
intensive care unit for 2 days and was discharged from the
hospital on postoperative day 6. However, superficial
wound dehiscence developed that involved the skin and
the subcutaneous tissue. This was treated with vacuum-
assisted closure (with the VAC Therapy system; KCI, Inc,
San Antonio, TX, USA), which facilitated wound healing
by secondary intention in 8 weeks.
Histopathologic examination of the excised tumor and
portion of the normal liver revealed a well-differentiated
11-cm HCC. There were focal areas of necrosis and hem-
orrhage from previous chemoradiation therapy, but there
was no evidence of microvascular invasion. In the normal
liver parenchyma, there was evidence of postemboliza-
tion effects, mainly focal areas of foreign body giant cell
reaction, but minimal fibrosis and no steatosis. All lymph
nodes were negative for malignancy. Currently, the
patient is doing well, with no evidence of recurrence 17
months after tumor resection.
Discussion
Several studies have found that obesity increases the risk
of complications and length of hospital stay and is inde-
pendently associated with increased mortality after elec-
tive abdominal surgery [10-13]. In contrast, a prospective
study of 6336 patients who underwent elective noncar-
diac surgery at a university hospital found that obesity
alone was not a risk factor for postoperative complica-
tions [14,15]. However, these findings were probably due
to the unusually low prevalence of major comorbidities in
the obese patients in these studies.
In a large study of 18,172 adult patients, including 3877
obese patients, who underwent LT in the US between
1988 and 1996, the rates of primary graft nonfunction
and of 1- and 2-year mortality were significantly higher in
the morbidly obese patients than in the other patients.
The authors of that study recommended that morbid
obesity (BMI > 35 kg/m2) be considered a relative con-
traindication for LT [16].
With regard to our morbidly obese patient (BMI, 56 kg/
m2) with a large HCC, during the initial surgical evalua-
tion, she was considered a high-risk candidate for
extended right hepatectomy because of her markedly
abnormal pulmonary function test results and the insuffi-
cient volume of the left lateral segment of her liver. We
believe that the neo-adjuvant treatment protocol we
implemented prevented tumor progression during the
aggressive weight-reduction program that the patient was
instructed to follow. This program was instituted because
pulmonary function test results and respiratory drive
parameters have been found to improve markedly after
weight loss [17].
The locoregional therapy protocol we implemented was
chosen on the basis of evidence that combination therapy
achieves a higher response rate than repeated TACE alone
in large HCCs [18,19]. Yttrium-90 microsphere injection
is a novel form of transarterial radiotherapy that has been
used increasingly for HCC as a single agent, and it has pro-
duced a good response rate [20,21]. To our knowledge, no
Table 2: Pulmonary function test results at initial evaluation and immediately before and after operation
Parameter Initial value Postoperative value
Forced vital capacity (L) 3.38 3.73
Forced expiratory volume in 1 second (L) 1.96 2.93
Maximum voluntary ventilation (L/min) 42 75
Vital capacity (L) 2.6 3.7
Total lung capacity (L) 4.1 5.9
Functional residual capacity (L) 1.6 2.3
Expiratory reserve volume (L) 0.02 0.06

World Journal of Surgical Oncology 2008, 6:100 http://www.wjso.com/content/6/1/100
Page 4 of 5
(page number not for citation purposes)
study has evaluated the use of radioembolization in con-
junction with other treatment modalities for any type of
malignant disease. However, evidence suggests that doxo-
rubicin hinders the repair of radiation-induced DNA dam-
age in HCC; thus, these treatments may have a synergistic
therapeutic effect [22].
As we anticipated, the tumor was found to be receiving its
blood supply from both branches of the hepatic artery. To
prevent ischemic injury to segments II and III of the left
lobe, we avoided injecting the embolization particles
through the left hepatic artery that supplied the lateral
aspect of the tumor. This might explain the tumor's failure
to respond despite repeated treatments. On the other
hand, selective injection into the middle and right hepatic
arteries might have spared segments I, II, and III the
adverse effects of chemoradiation treatment that were
seen in non-tumorous segments of the right lobe.
Preoperative portal vein embolization is becoming a
standard technique for inducing compensatory hypertro-
phy of the remaining liver and improving the safety and
rate of resectability in patients with small-for-size rem-
nant livers [23,24]. Furthermore, sequential preoperative
arterial and portal venous embolization can induce tumor
necrosis and hypertrophy of the normal liver, which allow
safe resection and longer recurrence-free survival [25,26].
We would have continued the locoregional therapy had
there been evidence of tumor response. On the other
hand, if the tumor had progressed, we would have added
systemic therapy, such as administering the multikinase
inhibitor sorafenib, to the treatment protocol. The deci-
sion to proceed with surgical resection was based on the
tumor's lack of response and, more importantly, on the
improved pulmonary function and reduced metabolic
syndrome that resulted from the successful weight-reduc-
tion program the patient followed during locoregional
treatment.
Conclusion
To reduce the risks that major liver resection poses in mor-
bidly obese patients with significant comorbidity, we sug-
gest implementing a dietary weight-reduction and exercise
program to improve the performance status of these
patients before resection. While this program is underway,
regional therapy can be implemented to prevent the
tumor from progressing to the point of inoperability. Por-
tal vein embolization may be required before resection to
increase the volume of the remnant liver and to reduce the
risk of liver failure and other postoperative complications.
We believe that further studies that include large numbers
of patients are needed to determine the upper limit of BMI
for performing extensive liver resection safely in morbidly
obese patients.
List of abbreviations
AFP: Alpha-Fetoprotein; BMI: Body Mass Index; CT: Com-
puted Tomography; HCC: Hepatocellular Carcinoma; LT:
Liver Transplantation; PVE: Portal Vein Embolization.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
OB: Performed the operation, devised the therapeutic
plan, and wrote the manuscript. MS: Performed the TACE;
helped in drafting the manuscript. BT: Performed the
TACE and Y-90 Sir-Sphere treatment, and helped in draft-
ing the manuscript. JF: Performed the portal vein emboli-
zation and TACE, and helped in drafting the manuscript.
CFO: Helped in drafting the manuscript. RPW: Co-sur-
geon during the operation; helped in designing the thera-
peutic plan, and proofread the manuscript.
Consent
Written informed consent was obtained from the patient
for publication of this case report and any accompanying
images. A copy of the written consent is available for
review by the Editor-in-Chief of this journal.
Acknowledgements
Stephen N. Palmer, PhD, ELS, contributed to the editing of this manuscript.
Dr. Palmer is an employee of the Texas Heart Institute at St. Luke's Epis-
copal Hospital.
References
1. The Surgeon General's Call to Action to Prevent and Decrease Overweight
and Obesity Rockville, MD: U.S. Dept. of Health and Human Services;
2001.
2. Flegal KM, Carroll MD, Ogden CL, Johnson CL: Prevalence and
trends in obesity among US adults, 1999–2000. JAMA 2002,
288:1723-1727.
3. Choban PS, Flancbaum L: The impact of obesity on surgical out-
comes: a review. Journal of the American College of Surgeons 1997,
185:593-603.
4. Nair S, Cohen DB, Cohen C, Tan H, Maley W, Thuluvath PJ: Postop-
erative morbidity, mortality, costs, and long-term survival in
severely obese patients undergoing orthotopic liver trans-
plantation. American Journal of Gastroenterology 2001, 96:842-845.
5. Calle EE, Thun MJ, Petrelli JM, Rodriguez C, Heath CW Jr: Body-
mass index and mortality in a prospective cohort of U.S.
adults. New England Journal of Medicine 1999, 341:1097-1105.
6. Ong JP, Younossi ZM: Is hepatocellular carcinoma part of the
natural history of nonalcoholic steatohepatitis? Gastroenterol-
ogy 2002, 123:375-378.
7. Shimada M, Hashimoto E, Taniai M, Hasegawa K, Okuda H, Hayashi
N, Takasaki K, Ludwig J: Hepatocellular carcinoma in patients
with non-alcoholic steatohepatitis. Journal of Hepatology 2002,
37:154-160.
8. Braunfeld MY, Chan S, Pregler J, Neelakanta G, Sopher MJ, Busuttil
RW, Csete M: Liver transplantation in the morbidly obese.
Journal of Clinical Anesthesia 1996, 8:585-590.
9. Fujikawa T, Fujita S, Mizuno S, Shenkman E, Vogel B, Lipori P, Hem-
ming AW, Nelson D, Reed AI: Clinical and financial impact of
obesity on the outcome of liver transplantation. Transplanta-
tion Proceedings 2006, 38:3612-3614.
10. Bamgbade OA, Rutter TW, Nafiu OO, Dorje P: Postoperative
complications in obese and nonobese patients. World Journal
of Surgery 2007, 31:556-560.
Publish with Bio Med Central and every
scientist can read your work free of charge
"BioMed Central will be the most significant development for
disseminating the results of biomedical research in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
World Journal of Surgical Oncology 2008, 6:100 http://www.wjso.com/content/6/1/100
Page 5 of 5
(page number not for citation purposes)
11. Dominguez EP, Choi YU, Scott BG, Yahanda AM, Graviss EA,
Sweeney JF: Impact of morbid obesity on outcome of laparo-
scopic splenectomy. Surgical Endoscopy 2007, 21:422-426.
12. Newell MA, Bard MR, Goettler CE, Toschlog EA, Schenarts PJ,
Sagraves SG, Holbert D, Pories WJ, Rotondo MF: Body mass index
and outcomes in critically injured blunt trauma patients:
weighing the impact. Journal of the American College of Surgeons
2007, 204:1056-1061.
13. Pikarsky AJ, Saida Y, Yamaguchi T, Martinez S, Chen W, Weiss EG,
Nogueras JJ, Wexner SD: Is obesity a high-risk factor for lapar-
oscopic colorectal surgery? Surgical Endoscopy 2002, 16:855-858.
14. Dindo D, Muller MK, Weber M, Clavien PA: Obesity in general
elective surgery. Lancet 2003, 361:2032-2035.
15. Klasen J, Junger A, Hartmann B, Jost A, Benson M, Virabjan T, Hemp-
elmann G: Increased body mass index and peri-operative risk
in patients undergoing non-cardiac surgery. Obesity Surgery
2004, 14:275-281.
16. Nair S, Verma S, Thuluvath PJ: Obesity and its effect on survival
in patients undergoing orthotopic liver transplantation in
the United States. Hepatology 2002, 35:105-109.
17. El-Gamal H, Khayat A, Shikora S, Unterborn JN: Relationship of
dyspnea to respiratory drive and pulmonary function tests in
obese patients before and after weight loss. Chest 2005,
128:3870-3874.
18. Poon RT, Fan ST, Tsang FH, Wong J: Locoregional therapies for
hepatocellular carcinoma: a critical review from the sur-
geon's perspective. Annals of Surgery 2002, 235:466-486.
19. Rossi S, Garbagnati F, Lencioni R, Allgaier HP, Marchiano A, Fornari
F, Quaretti P, Tolla GD, Ambrosi C, Mazzaferro V, et al.: Percutane-
ous radio-frequency thermal ablation of nonresectable hepa-
tocellular carcinoma after occlusion of tumor blood supply.
Radiology 2000, 217:119-126.
20. Lau WY, Leung WT, Ho S, Leung NW, Chan M, Lin J, Metreweli C,
Johnson P, Li AK: Treatment of inoperable hepatocellular car-
cinoma with intrahepatic arterial yttrium-90 microspheres:
a phase I and II study. British Journal of Cancer 1994, 70:994-999.
21. Salem R, Lewandowski RJ, Atassi B, Gordon SC, Gates VL, Barakat O,
Sergie Z, Wong CY, Thurston KG: Treatment of unresectable
hepatocellular carcinoma with use of 90Y microspheres
(TheraSphere): safety, tumor response, and survival. Journal
of Vascular and Interventional Radiology 2005, 16:1627-1639.
22. Bonner JA, Lawrence TS: Doxorubicin decreases the repair of
radiation-induced DNA damage. Int J Radiat Biol 1990, 57:55-64.
23. Farges O, Belghiti J, Kianmanesh R, Regimbeau JM, Santoro R, Vilgrain
V, Denys A, Sauvanet A: Portal vein embolization before right
hepatectomy: prospective clinical trial. Annals of Surgery 2003,
237:208-217.
24. Truant S, Oberlin O, Sergent G, Lebuffe G, Gambiez L, Ernst O, Pru-
vot FR: Remnant liver volume to body weight ratio > or =
0.5%: a new cut-off to estimate postoperative risks after
extended resection in noncirrhotic liver. Journal of the American
College of Surgeons 2007, 204:22-33.
25. Aoki T, Imamura H, Hasegawa K, Matsukura A, Sano K, Sugawara Y,
Kokudo N, Makuuchi M: Sequential preoperative arterial and
portal venous embolizations in patients with hepatocellular
carcinoma. Archives of Surgery 2004, 139:766-774.
26. Ogata S, Belghiti J, Farges O, Varma D, Sibert A, Vilgrain V: Sequen-
tial arterial and portal vein embolizations before right hepa-
tectomy in patients with cirrhosis and hepatocellular
carcinoma. British Journal of Surgery 2006, 93:1091-1098.


























%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)