BioMed Central
Page 1 of 5
(page number not for citation purposes)
World Journal of Surgical Oncology
Open Access
Case report
Pyoderma gangrenosum after totally implanted central venous
access device insertion
Ihsan Inan*1, Patrick O Myers1, Rolf Braun2, Monica E Hagen1 and
Philippe Morel1
Address: 1Visceral Surgery Unit, Department of Surgery, Geneva University Hospital, Rue Micheli-du-Crest 24, CH-1211 Geneva, Switzerland and
2Dermatology Department, Geneva University Hospital, Rue Micheli-du-Crest 24, CH-1211 Geneva, Switzerland
Email: Ihsan Inan* - ihsan.inan@hcuge.ch; Patrick O Myers - patrick.myers@hcuge.ch; Rolf Braun - rolf.braun@hcuge.ch;
Monica E Hagen - monica.hagen@hcuge.ch; Philippe Morel - philippe.morel@hcuge.ch
* Corresponding author
Abstract
Background: Pyoderma gangrenosum is an aseptic skin disease. The ulcerative form of pyoderma
gangrenosum is characterized by a rapidly progressing painful irregular and undermined bordered
necrotic ulcer. The aetiology of pyoderma gangrenosum remains unclear. In about 70% of cases, it
is associated with a systemic disorder, most often inflammatory bowel disease, haematological
disease or arthritis. In 25–50% of cases, a triggering factor such as recent surgery or trauma is
identified. Treatment consists of local and systemic approaches. Systemic steroids are generally
used first. If the lesions are refractory, steroids are combined with other immunosuppressive
therapy or to antimicrobial agents.
Case presentation: A 90 years old patient with myelodysplastic syndrome, seeking regular
transfusions required totally implanted central venous access device (Port-a-Cath®) insertion.
Fever and inflammatory skin reaction at the site of insertion developed on the seventh post-
operative day, requiring the device's explanation. A rapid progression of the skin lesions evolved
into a circular skin necrosis. Intravenous steroid treatment stopped the necrosis' progression.
Conclusion: Early diagnosis remains the most important step to the successful treatment of
pyoderma gangrenosum.
Background
Patients undergoing totally implanted central venous
access device (TICVAD) insertion are frequently at risk of
infection, firstly by implanting foreign material, which
can be colonized and difficult to treat, secondly because
the underlying disease often is associated with a decreased
immune response such as metastatic malignant diseases
and haemopathies. The first aetiology of inflammatory
ulcerative skin lesions associated with TICVAD insertion
is thus usually assumed to be bacterial infection [1]. How-
ever, the differential diagnosis of these skin lesions is
quite wide, and must be considered in all its breadth
when managing such lesions after TICVAD insertion. One
can name bacterial (including mycobacterial) skin infec-
tions, necrotizing fasciitis, deep mycosis, chronic herpes
simplex infection, vasculitis (Wegener's disease),
antiphospholipid-antibody syndrome, parasitic infection
(cutaneous leishmaniasis or amebiasis), halogene derma-
Published: 6 March 2008
World Journal of Surgical Oncology 2008, 6:31 doi:10.1186/1477-7819-6-31
Received: 9 February 2008
Accepted: 6 March 2008
This article is available from: http://www.wjso.com/content/6/1/31
© 2008 Inan et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Surgical Oncology 2008, 6:31 http://www.wjso.com/content/6/1/31
Page 2 of 5
(page number not for citation purposes)
titis, coumarine necrosis or injection drug abuse with sec-
ondary infection as most frequent causes of such
lesions[2,3]. Pyoderma gangrenosum (PG) is a rare, asep-
tic skin disease, which should be considered in the differ-
ential diagnosis. To our knowledge, we report the first case
of PG after TICVAD insertion and discuss the difficulties
in management that such cases represent.
Case presentation
A 90 year-old patient in good general health, known for a
myelodysplastic syndrome with refractory anaemia and
myelofibrosis, became transfusion and thrombapheresis
dependent, requiring implantation of a right subclavian
TICVAD. Thereafter he developed dyspnoea and a fever of
38.6°C, motivating hospitalisation at the 7th postopera-
tive day. An ischemic left cardiac decomposition was diag-
nosed, in the context of positive troponins, anterolateral
ischemic signs on the ECG and severe anaemia (haemo-
globin 68 g/l). Important skin inflammation with central
necrotic ulceration and violet coloration of the edges was
noted on the site of the TICVAD (figure 1 and 2). Labora-
tory investigations revealed an inflammatory state (leuco-
cytosis at 11,8 G/l, non segmented neutrophils 8%, C-
Reactive protein 175 mg/l). The TICVAD was removed on
the 8th post-operative day, cultures were taken and wide-
spectrum antibiotics (cefepime and vancomycine) were
introduced. Because of persistent fever and progressive
renal failure, the antibiotics were changed to imipenem
and teicoplanine. Cultures showed that pathogenic bacte-
ria are not involved.
Despite these antibiotics, a fever and an inflammatory
state persisted. The skin necrosis progressed rapidly
around the TICVAD explanation site to the right upper
chest wall (figure 3). A biopsy of the necrosis's edge
revealed non-specific inflammation, diagnosis of PG is
retained on clinical evolution. Corticosteroid therapy was
started, improving both the skin lesions and systemic
inflammatory signs.
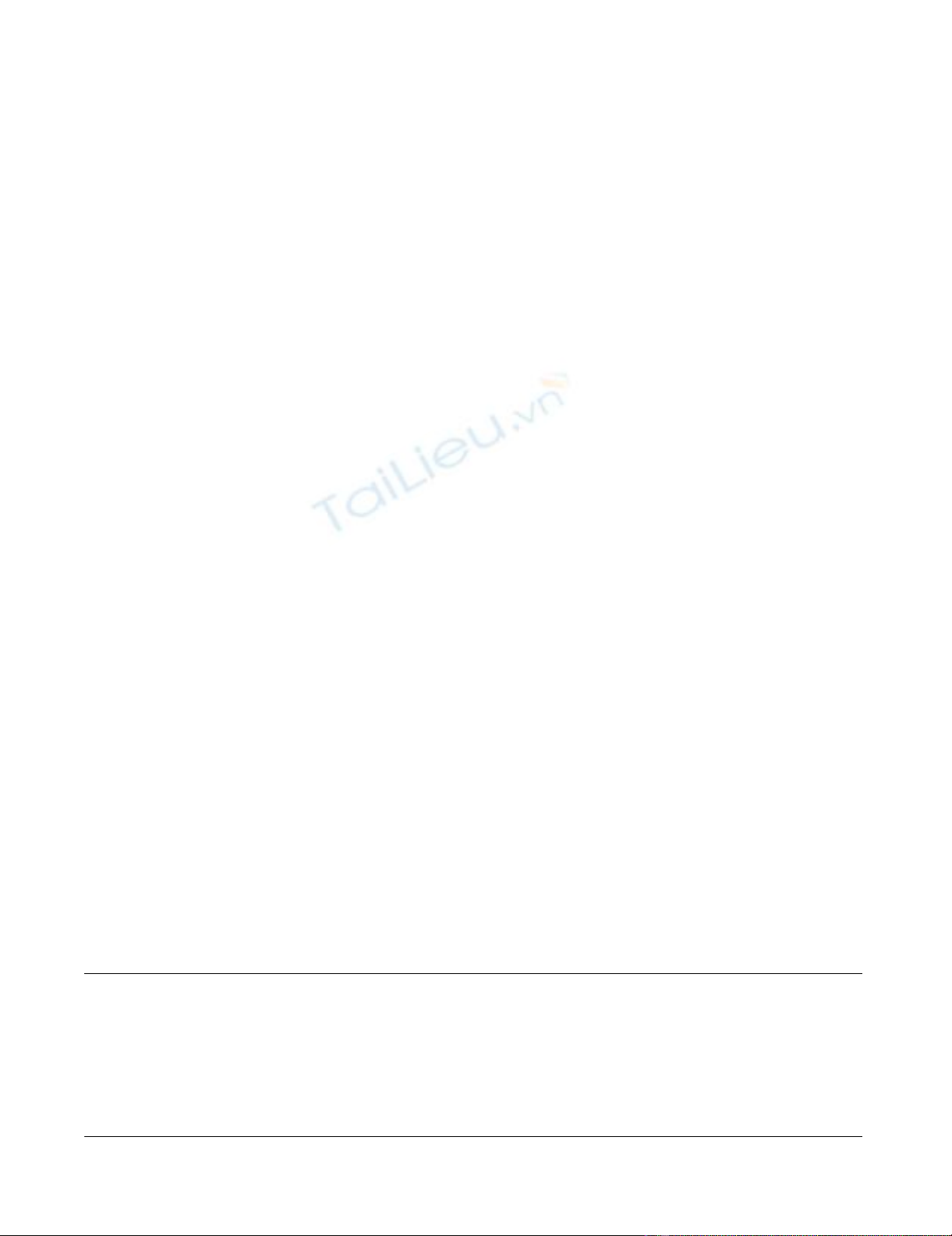
5 days post extraction, diagnostic of PG retainedFigure 3
5 days post extraction, diagnostic of PG retained.
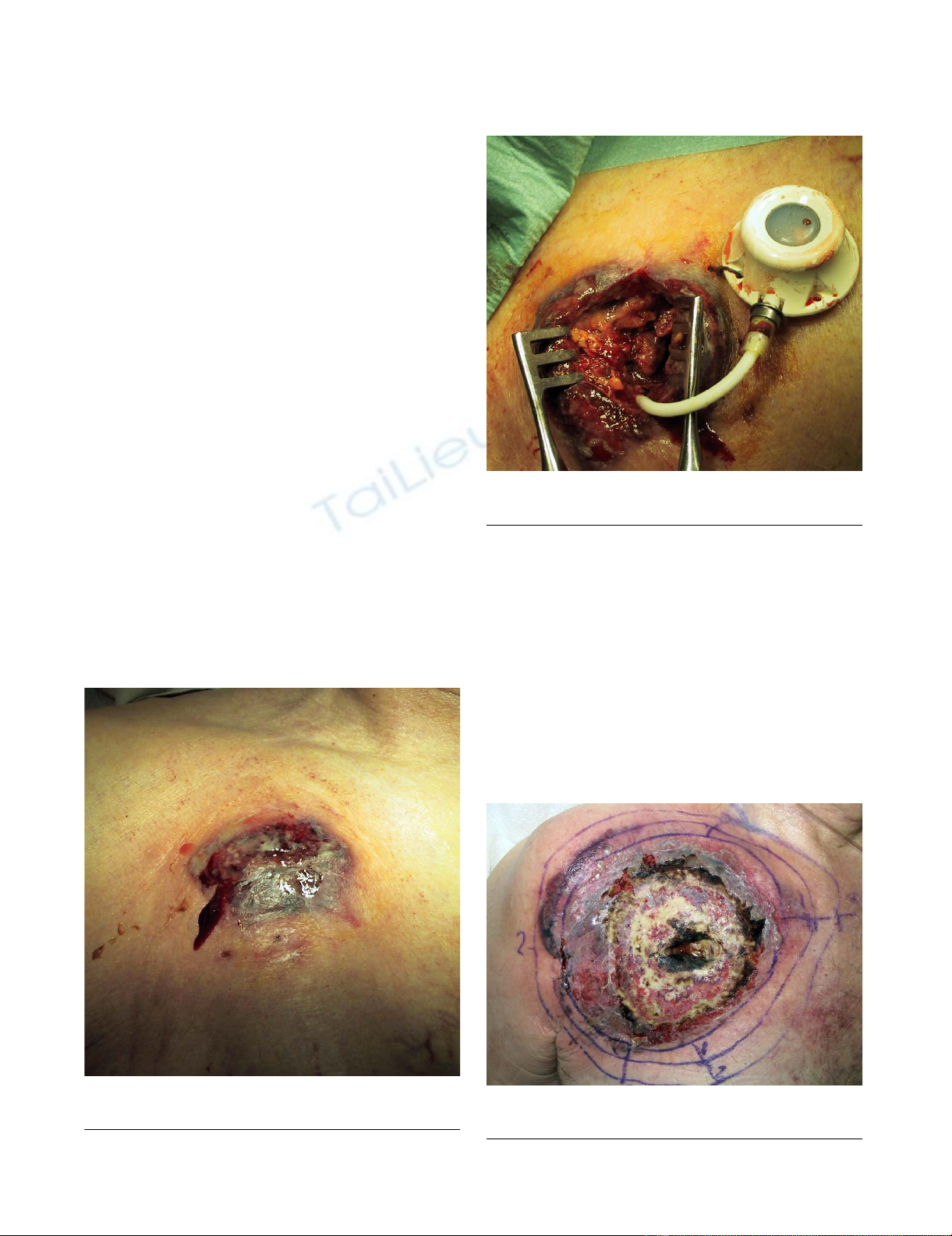
7 days after TICVAD implantationFigure 1
7 days after TICVAD implantation.
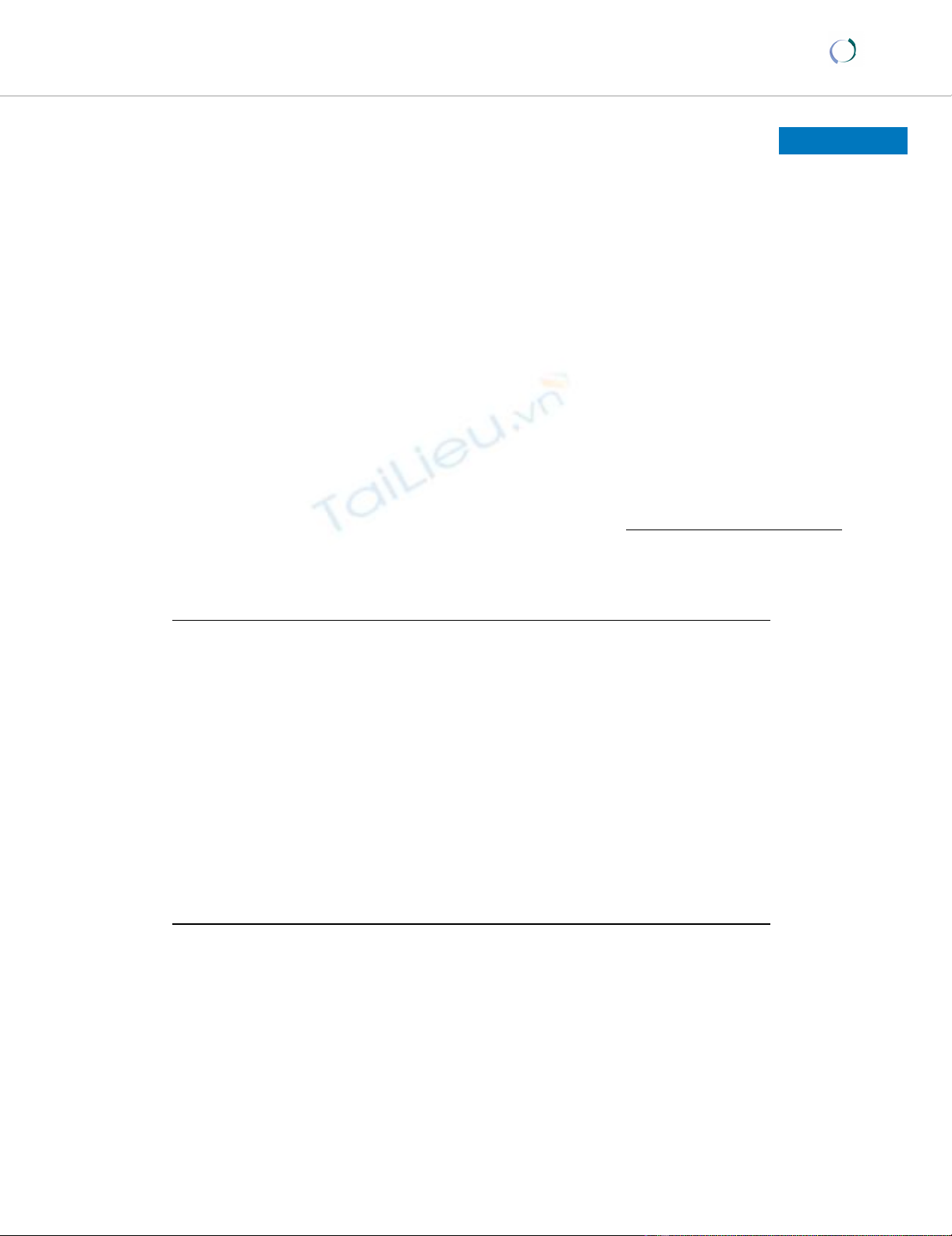
During the extraction of TICVADFigure 2
During the extraction of TICVAD.
World Journal of Surgical Oncology 2008, 6:31 http://www.wjso.com/content/6/1/31
Page 3 of 5
(page number not for citation purposes)
Unfortunately, the patient developed acute anuric renal
failure of mixed aetiology (systemic inflammatory
response syndrome, toxic to vancomycine and pre-renal).
The patient died on the 15th post-operative day.
Of note, the patient was hospitalised in our institution
one year earlier for a rapidly growing necrosis, bordered
with a violet coloration, of the distal phalanx of the right
index finger after a minor trauma. Despite antibiotic treat-
ment and successive debridements and amputations, the
last of which was at the metacarpo-carpal joint, the ulcer
progressed. Cultures remained sterile. The hand healed 6
months later with conservative treatment. The diagnosis
of PG was not evoked at that time.
Discussion
Pyoderma gangrenosum is an aseptic skin disease. The
aetiology of pyoderma gangrenosum is unclear. Pyo-
derma gangrenosum was first reported in 1924 following
drainage of an abdominal abscess [4] and formally
described in 1930 [5] as an unusual skin eruption
reported in five cases, four of which had chronic ulcerative
colitis. It was given such a name because the authors
believed that streptococcal infection was a significant
component leading to secondary cutaneous gangrene.
This was shown not to be relevant, although the cause of
PG remains obscure, most probably an immunological
anomaly of the hyperergic reaction type. IL-8, a potent
leukocyte chemotactic agent, has been shown to be over-
expressed in PG ulcers and to induce similar ulceration in
human skin xenografts transfected with recombinant
human IL-8[6]. IL-16, a neutrophil chemotactic agent, has
also been implicated[3,7]. The factors inciting or main-
taining these abnormalities are unclear but likely are mul-
tiple, mixing genetic predisposition, undefined infectious
agents or paraneoplastic or paraimmune phenomena[3].
PG is a diagnosis of exclusion[8]. The distinctive clinical
features of PG are apparent enough to permit the diagno-
sis of most cases[3], comprising in it's classic form a bur-
rowing ulcer with an irregular margin and ragged purple-
red overhanging edge. Lesions can be solitary or multiple,
chronic or recurrent, most often localized on the legs, par-
ticularly in the pretibial region, or, in patients who have
undergone colectomy for inflammatory bowel disease
(IBD), around a colostomy. The initial lesion starts with
an inflammatory papule or follicular pustule, surrounded
by erythema or a haemorrhagic bulla with an erythema-
tous base. It evolves into an ulcer with a purulent base and
a violaceous border, which progresses outwards. Ulcers
heal leaving an atrophic-pigmented and cribriform
scar.[3,9]
PG has been classified into four different types: ulcerous,
pustulous, vegetans and bullous[3,10] (Table 1).
Extracutaneous manifestations are also described, most
frequently pulmonary, although all organs can be
affected. Some patients develop fever asthenia, myalgias,
and arthralgias. PG can lead to multiorgan system failure
in the context of severe inflammatory response syndrome.
The histopathological features of PG are relatively aspe-
cific, revealing important neutrophilic infiltrate, haemor-
rhage and necrosis of the epidermis, but are useful in
ruling out other causes of ulceration[3,9].
Approximately fifty to 70% of cases are associated with a
systemic disease, usually IBD, arthritis or haematological
disorders. Both type and severity of associated disease is
important on the prognosis of PG. Most frequent haema-
tological disorders associated include acute myeloblastic
leukaemia, "hairy cell" leukaemia, myelodisplasic syn-
drome, myelofibrosis and IgA monoclonal gammopathy.
Most of the time successful treatment of associated disease
results in remission of PG. Some cytokines such as granu-
locyte colony-stimulating factor, interferons and antipsy-
chotic drugs have been shown to induce PG.[2,9]
Pathergy, i.e. lesions developing at the site of minor
trauma or surgery, is observed in 25–50% of cases[11]. PG
has been observed on the incision site after digestive sur-
gery, hernia repair, gynaecologic surgery, breast surgery,
plastic surgery and cardiovascular surgery.
Diagnostic exams should include skin biopsy of the bor-
der of the skin lesions for histology and culture (including
Table 1: Classification of PG
Ulcerous PG The most common form is the ulcerous type. It is rapidly progressive, severely painful and characterized by a necrolytic,
mucopurulent deep ulcer with an undermined, violaceous, oedematous livid border. PG ulcer is a dynamic process, rapidly
destroying skin tissue, producing a liquefactive necrosis. It is associated with arthritis (37%), IBD (30%), hematological malignancies,
multiple myeloma, paraproteinema and other conditions. Aggressive immunosuppressant treatment is indispensable.
Pustulous PG Pustulous PG is characterized by multiple lesions with inflammatory borders. It is strongly associated with IBD. Upon remission of
IBD, skin lesions also improve.
Vegetans PG Vegetans PG is solitary, slowly progressive form of PG, characterized by superficial ulcerations with defined borders, sometimes
presenting exophytic growth. Less aggressive systemic or topical treatment is usually sufficient.
Bullous PG Bullous PG is characterized by painful superficial bullae with progressive ulceration and erythematous borders. It is associated with
myeloproliferative syndromes and has a poor prognosis if associated with leukemia. Systemic immunosuppression is necessary.

World Journal of Surgical Oncology 2008, 6:31 http://www.wjso.com/content/6/1/31
Page 4 of 5
(page number not for citation purposes)
yeast, parasites and mycobacteria), complete blood count
(and marrow aspiration/biopsy if pathological), sedimen-
tation rate, c-reactive protein, renal and hepatic function,
serum and urinary protein electrophoresis and immune-
lectrophoresis, anticardiolipid antibodies, VDRL, p- and
c-ANCA, cryoglobulines, coagulation, chest x-ray and
endoscopic examination of colon and rectum. [9]
The case that we report demonstrates how wide the differ-
ential diagnosis of inflammatory ulcerative skin lesions is,
and how difficult is to diagnose pyoderma gangrenosum.
Skin lesions were attributed to bacterial infection due to
recent TICVAD operation. PG was considered because of
persistent cultures showing that pathologic bacteria are
not involved and absence of lesion improvement under
different antibiotics. Despite the non-specific biopsy, the
diagnosis of PG retained on clinical basis and treatment
was started. Unfortunately, the patient developed such an
extensive inflammatory response associated with toxic
renal failure that death was inevitable at this stage. The
recurrent skin necrosis of the right hand a year prior
should retrospectively be attributed to PG. A history of
previous ulcerative skin lesions of unknown aetiology
resulting in amputation in a patient presenting character-
istic ulcerative lesions after TICVAD implantation should
make one evoke the diagnosis of PG.
The aim of the therapy is to prevent the progression of the
ulcers, encourage reepithelisation and decrease pain[12].
There is no specific or standard therapeutic strategy for
PG. Despite the large number of treatment proposed, con-
trolled clinical trials are lacking [2]. Immunosuppression
is the basis of treatment; corticosteroids and cyclosporine
are the most commonly used drugs. Sequence and combi-
nation of topical and systemic treatment is empirical and
frequently depends on local experience[10].
Topical treatment is generally insufficient as mono-
therapy and used as supportive treatment for systemic
treatment[12]. Topical treatment includes topical or int-
ralesional corticosteroids, tacrolimus ointment, intrale-
sional cyclosporine, topical 5 aminosalicylic acid,
nitrogen mustard or 0,5% nicotine cream[2,13].
Systemic treatment is started in most of the cases with cor-
ticosteroids (e.g., methylprednisolone 0.5–1 mg/kg/d) or
cyclosporine (e.g., 5 mg/kg/d) alone and considered as
first-line therapy. Stabilization of the disease is usually
achieved within 24 hours. For cases refractory to first line
therapy with concomitant inflammatory bowel disease,
second line treatment includes biological response modi-
fiers and immunomodulatory therapy. Tacrolimus, tha-
lidomide, azathioprine, dapsone, mycophenolate mofetil
and infliximab are shown to be effective in case reports or
small series. In cases without associated disease, intrave-
nous immunoglobulins, granulocyte and monocyte
adsorption apheresis plasmapheresis and cyclophospha-
mide treatment are also reported to be effective.[2]
Debridement or necrosectomy in postoperative PG is con-
traindicated [11]. Elective surgery for other indications
should be deferred, and if unavoidable, it should be per-
formed in conjunction with systemic PG therapy[2].
Conclusion
PG represents a diagnostic challenge. In the presence of a
patient with cutaneous inflammatory and necrotizing
lesions one must consider PG as a differential diagnosis.
Early diagnosis remains the most important step to the
successful treatment of pyoderma gangrenosum
Competing interests
The author(s) declare that they have no competing inter-
ests.
Authors' contributions
II carried out the surgical care of the patient and the fol-
low-up during the treatment, realised the illustration and
drafted the manuscript. POM participated to manuscript
draft and literature research. RB participated in the follow-
up of the patient, diagnosis of the disease and treatment
as well as manuscript draft on dermatologic aspect. MEH
participated to manuscript draft and literature research.
PM encouraged the case report, participated in its prepa-
ration and helped to draft the manuscript. All authors
read and approved the final manuscript.
Acknowledgements
Permission was obtained from the local ethics committee for publication of
this case report.
Special thanks to Dr K-M. Djebaili and Dr N. Exer for care given to the
patient during the treatment.
References
1. Hachem R, Raad I: Prevention and management of long-term
catheter related infections in cancer patients. Cancer Invest
2002, 20:1105-1113.
2. Reichrath J, Bens G, Bonowitz A, Tilgen W: Treatment recom-
mendations for pyoderma gangrenosum: an evidence-based
review of the literature based on more than 350 patients. J
Am Acad Dermatol 2005, 53:273-283.
3. Su WP, Davis MD, Weenig RH, Powell FC, Perry HO: Pyoderma
gangrenosum: clinicopathologic correlation and proposed
diagnostic criteria. Int J Dermatol 2004, 43:790-800.
4. Cullen TS: A progressively enlarging ulcer of the abdominal
wall involving skin and fat, following drainage of an abdomi-
nal abscess apparently from appendiceal origin. Surg Gynecol
Obstet 1924, 38:579-582.
5. Brunsting L, Goeckerman W, O'Leary P: Pyoderma gangreno-
sum: clinical and experimental observations in five cases
occuring in adults. Arch Dermatol 1930, 22:655-680.
6. Oka M, Berking C, Nesbit M, Satyamoorthy K, Schaider H, Murphy G,
et al.: Interleukin-8 overexpression is present in pyoderma
gangrenosum ulcers and leads to ulcer formation in human
skin xenografts. Lab Invest 2000, 80:595-604.
Publish with BioMed Central and every
scientist can read your work free of charge
"BioMed Central will be the most significant development for
disseminating the results of biomedical research in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
World Journal of Surgical Oncology 2008, 6:31 http://www.wjso.com/content/6/1/31
Page 5 of 5
(page number not for citation purposes)
7. Yeon HB, Lindor NM, Seidman JG, Seidman CE: Pyogenic arthritis,
pyoderma gangrenosum, and acne syndrome maps to chro-
mosome 15q. Am J Hum Genet 2000, 66:1443-1448.
8. Weenig RH, Davis MD, Dahl PR, Su WP: Skin ulcers misdiagnosed
as pyoderma gangrenosum. N Engl J Med 2002, 347:1412-1418.
9. Callen JP: Pyoderma gangrenosum. Lancet 1998, 351:581-585.
10. Brooklyn T, Dunnill G, Probert C: Diagnosis and treatment of
pyoderma gangrenosum. BMJ 2006, 333:181-184.
11. Bennett ML, Jackson JM, Jorizzo JL, Fleischer AB Jr, White WL, Callen
JP: Pyoderma gangrenosum. A comparison of typical and
atypical forms with an emphasis on time to remission. Case
review of 86 patients from 2 institutions. Medicine (Baltimore)
2000, 79:37-46.
12. Ehling A, Karrer S, Klebl F, Schaffler A, Muller-Ladner U: Therapeu-
tic management of pyoderma gangrenosum. Arthritis Rheum
2004, 50:3076-3084.
13. Patel GK, Rhodes JR, Evans B, Holt PJ: Successful treatment of
pyoderma gangrenosum with topical 0.5% nicotine cream. J
Dermatolog Treat 2004, 15:122-125.


























%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)