BioMed Central
Page 1 of 4
(page number not for citation purposes)
World Journal of Surgical Oncology
Open Access
Case report
Small cell carcinoma of the appendix
Anna M O'Kane1, Mark E O'Donnell*1, Rajeev Shah2, Declan P Carey1 and
Jack Lee1
Address: 1Department of Surgery, Belfast City Hospital, Lisburn Road, Belfast BT9 7AB. Northern Ireland, UK and 2Department of Histopathology,
Belfast City Hospital, Lisburn Road, Belfast BT9 7AB. Northern Ireland, UK
Email: Anna M O'Kane - okaneam@doctors.org.uk; Mark E O'Donnell* - modonnell904@hotmail.com;
Rajeev Shah - rajeevshah12@yahoo.co.uk; Declan P Carey - declan.carey@belfasttrust.hscni.net; Jack Lee - jacklee@doctors.org.uk
* Corresponding author
Abstract
Background: An extrapulmonary small cell carcinoma is a rare condition. It has similar histological
features to pulmonary small cell carcinoma and is equally aggressive.
Case presentation: We present the case of a 60-year-old woman who presented with right
upper quadrant pain. Computerised tomography revealed an appendiceal lesion and multiple liver
metastases. Exploratory laparotomy and right hemicolectomy was performed with
histopathological analysis confirming a primary small cell carcinoma of her appendix.
Conclusion: This is the first reported case of a pure extrapulmonary carcinoma arising from the
appendix.
Background
Extrapulmonary small cell carcinomas (ESC) are rare.
Many different sites of origin have been described includ-
ing kidney, bladder, prostate, endometrium, salivary
glands, nasal sinuses and intestinal tract [1-5]. Primary
colonic ESC remains the rarest and most aggressive. There
is an equal sex distribution with a preponderance for mid-
dle aged patients. We present a case of a 60-year old
female with a primary small cell carcinoma of the appen-
dix with liver metastasis.
Case presentation
A 60-year-old female was admitted with a 4-day history of
right upper quadrant pain. She was treated with oral anti-
biotics for suspected acute cholecystitis. She had a past
medical history of Type-2 diabetes and hypertension. She
was a non-smoker. The patient had no fever, sweating or
rigors but described similar intermittent pain with associ-
ated nausea and vomiting over the preceding 6-weeks. On
examination, the patient was comfortable and well nour-
ished. Her clinical parameters (pulse and blood pressure)
were normal and she was apyrexic. Abdominal examina-
tion revealed right upper quadrant tenderness with a pal-
pable liver edge. There were no other masses or
organomegaly.
Haematological analyses showed a haemoglobin level of
13.9 g/dl, white cell count 10.8 × 109/l and C-reactive pro-
tein 19 mg/L. All other indices were normal as were the
plain chest and abdominal X-rays. An abdominal ultra-
sound showed a markedly abnormal liver appearance
with multiple hypoechoic lesions suggestive of multiple
metastases. The remainder of the biliary tree was normal.
A contrast-enhanced computerised tomography (CT) scan
of the chest, abdomen and pelvis confirmed multiple liver
metastases within both lobes of the liver but also a 6 × 7
Published: 15 January 2008
World Journal of Surgical Oncology 2008, 6:4 doi:10.1186/1477-7819-6-4
Received: 7 September 2007
Accepted: 15 January 2008
This article is available from: http://www.wjso.com/content/6/1/4
© 2008 O'Kane et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Surgical Oncology 2008, 6:4 http://www.wjso.com/content/6/1/4
Page 2 of 4
(page number not for citation purposes)
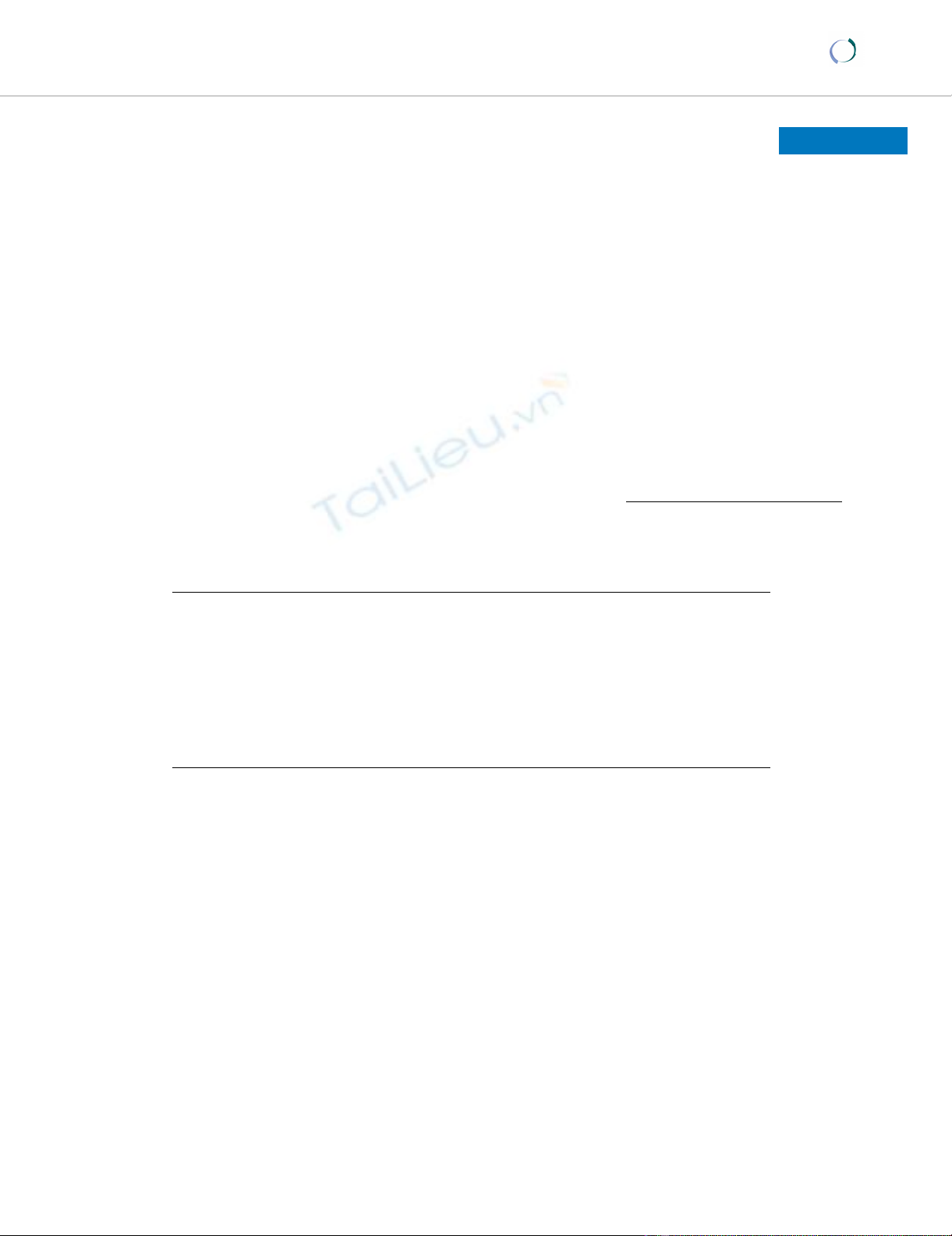
cm tumour mass in the right iliac fossa (Figures 1 &2).
There was associated lymphadenopathy extending
through the ileo-colic branch of the superior mesenteric
artery and further large lymph nodes measuring up to 1.9
cms in diameter in the aorto-caval and para-aortic regions.
Although the lesion was separate from the ileo-caecal
valve, radiological imaging suggested an appendiceal or
caecal origin. Further extrinsic pressure to the distal third
of the right ureter was present with mild hydronephrosis.
No lung parenchymal abnormality was identified.
Gastrointestinal investigation with colonoscopy was
planned but cancelled due to deteriorating symptomatol-
ogy with conservative treatment. Laparotomy revealed a
large tumour mass which appeared to originate from the
ascending colon. This was adherent to but not invading
the right ureter and lateral abdominal wall. Liver metas-
tases and multiple enlarged lymph nodes along the ileo-
colic branch of the superior mesenteric artery were also
identified. Due to the involvement of surrounding struc-
tures and a suspected caecal origin a right hemicolectomy
was performed with a primary ileo-colic anastomosis. The
right ureter was preserved as the tumour was dissected free
of both the ureter and lateral abdominal wall. No syn-
chronous colorectal tumour was identified during surgery.
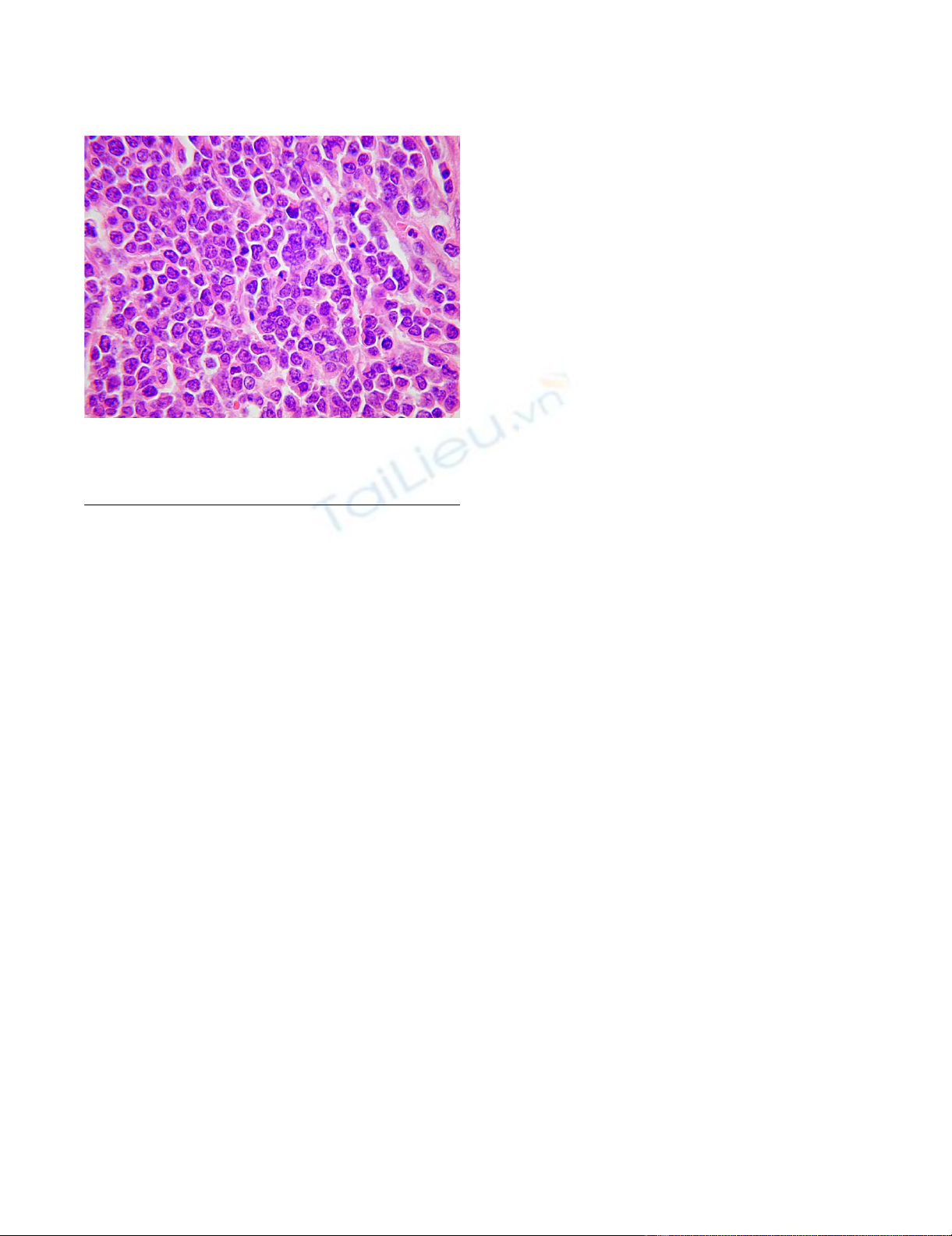
Macroscopic examination showed that the tumour had
replaced the appendix without caecal involvement (Figure
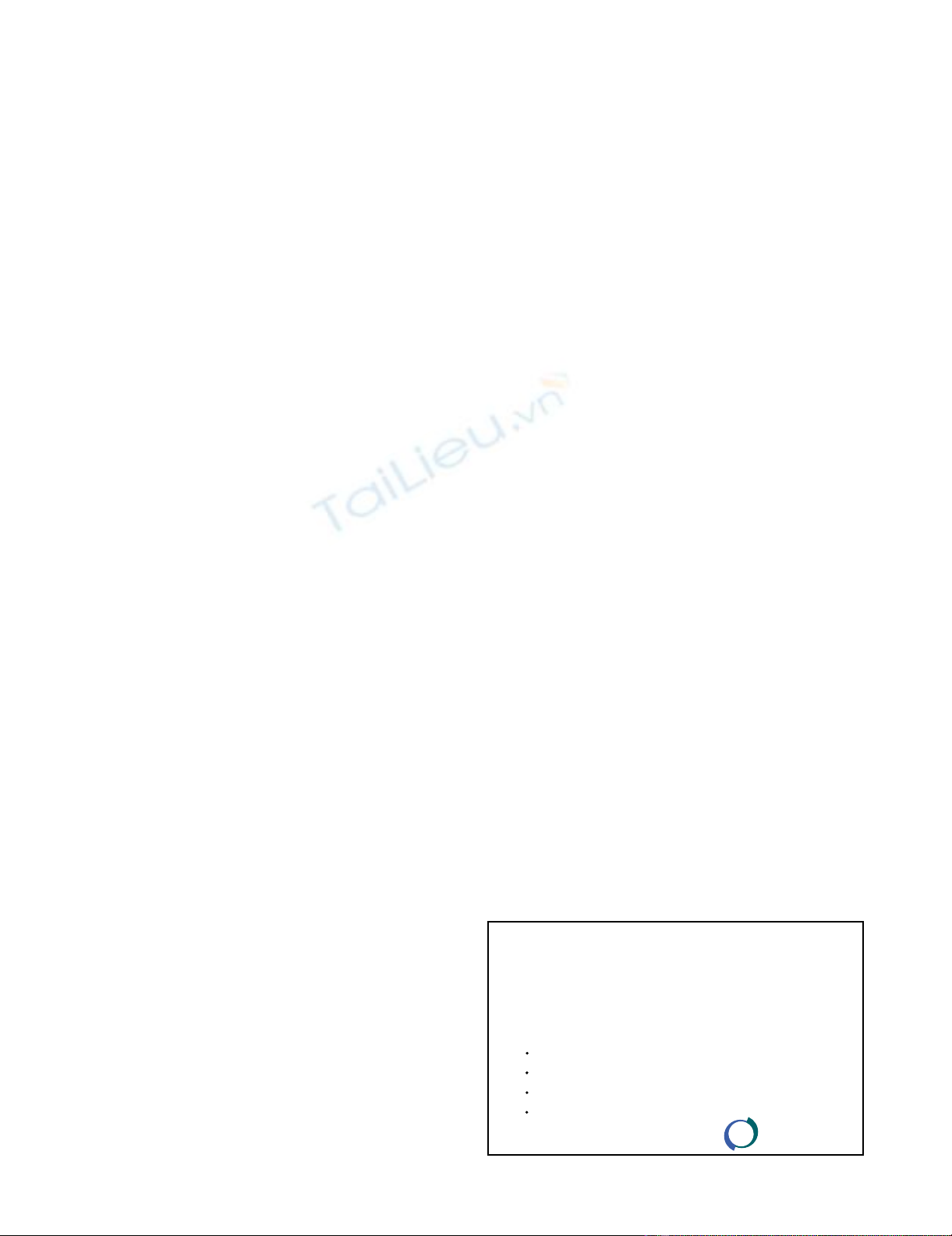
3). Histological examination showed a small cell carci-
noma tumour composed of small cells with round to
ovoid nuclei, dispersed chromatin, scanty cytoplasm and
abundant mitoses (Figure 4). The tumour had extended
through the peritoneum and involved the surrounding
adipose tissue replacing the entire appendiceal mucosa.
There was extensive lymphovascular invasion and meta-
static involvement of regional lymph nodes. Immunohis-
tochemistry demonstrated positivity for the epithelial
markers CAM 5.2 and AE1/AE3 and the neuroendocrine
markers PGP 9.5, synaptophysin and TTF1. Ki-67 staining
index was approximately 90%. Tumours cells were nega-
tive for cytokeratin 7, cytokeratin 20, CD 45 (LCA),
desmin, WT-1, CD 56, chromogranin and CD 99. The
morphology and immunohistochemical features were in
Macroscopic image demonstrating the extrapulmonary small cell carcinoma which had surrounded and replaced the appendix without caecal involvementFigure 3
Macroscopic image demonstrating the extrapulmonary small
cell carcinoma which had surrounded and replaced the
appendix without caecal involvement.
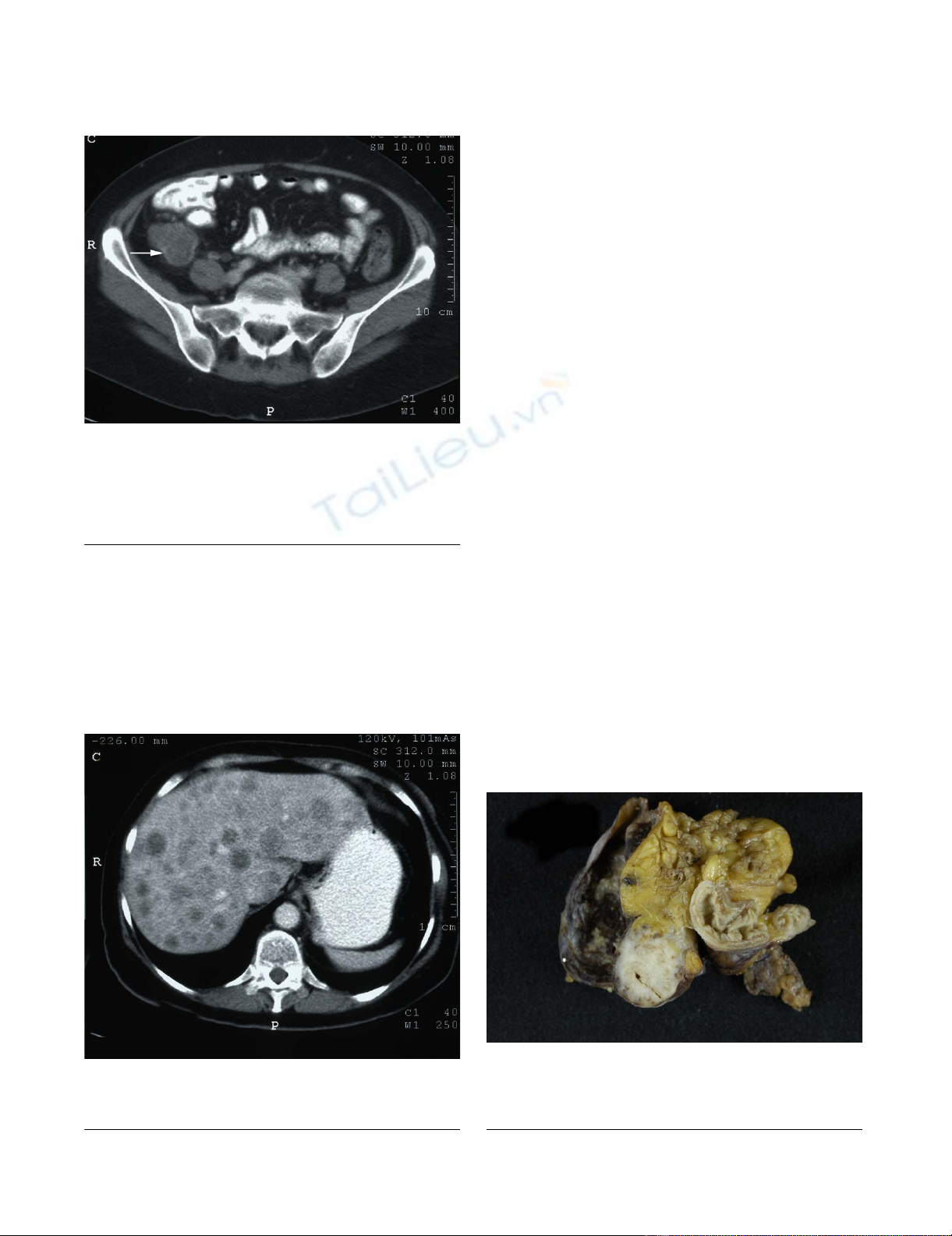
Contrast-enhanced computerised tomography scan of the abdomen demonstrating multiple liver metastasesFigure 2
Contrast-enhanced computerised tomography scan of the
abdomen demonstrating multiple liver metastases.
Contrast-enhanced computerised tomography scan of the abdomen demonstrating a 6 cm × 7 cm tumour mass in the right iliac fossa (white arrow)Figure 1
Contrast-enhanced computerised tomography scan of the
abdomen demonstrating a 6 cm × 7 cm tumour mass in the
right iliac fossa (white arrow). Although the tumour mass
was inseparable from the lower pole of the caecum, it
appeared separate from the ileo-caecal valve.
World Journal of Surgical Oncology 2008, 6:4 http://www.wjso.com/content/6/1/4
Page 3 of 4
(page number not for citation purposes)
keeping with a neuroendocrine carcinoma of small cell
type. In the absence of an identified pulmonary tumour, a
diagnosis of primary appendiceal small cell carcinoma
was made.
She made an uneventful surgical recovery and was trans-
ferred to the oncology department 12-days after surgery
for palliative chemotherapy. The patient developed a right
flank abscess after receiving one cycle of carboplatin. The
abscess was drained percutaneously. Subsequently the
patient was referred to the palliative care team and passed
away 2-months after surgery. A post mortem was not per-
formed.
Discussion
Undifferentiated small cell carcinoma (SCC) is an aggres-
sive lung tumour accounting for 15% of all lung cancers
[1]. Extrapulmonary small cell carcinomas (ESC) in com-
parison are rare with an incidence between 0.1–0.4% of
all cancers [2]. Approximately 2.5% of all SCC's arise in
extrapulmonary sites such as the salivary glands, pharynx,
larynx, nasal sinuses, pancreas, oesophagus, colon, rec-
tum, skin and cervix [2-5]. Colorectal ESCs are rare with
an incidence of 0.3% of all colorectal cancers and like SCC
of the lung, are aggressive malignancies with early metas-
tasis and have an overall 5-year survival of 13% [6]. Kim
et al (2004) reported a 12.5% incidence of colorectal ESC
with 3 patients affected from a retrospective review of 24
patients with ESC [7].
Age and sex distribution for ESC are similar to that seen in
adenocarcinoma of the colon [6]. Although smoking is
clearly implicated in the formation of pulmonary SCC, its
association with ESC is not clearly documented. This
patient was a non-smoker but there was a family history
of lung cancer with an elderly brother who died in his fif-
ties. The type of lung cancer affecting the patient's brother
was not determined and therefore it is unclear whether
her family history of lung cancer had a causative role
either.
SCC is thought to originate from neuroendocrine cells,
which are found in the epithelium of many mucosal sur-
faces including the gastrointestinal tract [6]. Despite evi-
dence of neuroendocrine involvement, the origin of ESC
is still unclear as development from undifferentiated air-
way epithelium has also been suggested along with the
amine precursor uptake and decarboxylation (APUD) sys-
tem hypothesis which proposes a common ancestral cell
derived from the neural crest, which then migrates to var-
ious epithelial tissues and sites within the body [8,9].
Histopathological diagnosis can be confirmed by the clas-
sic appearance of small round to oval shaped cells with a
finely granular and hyperchromatic nucleus, inconspicu-
ous nucleoli and scanty cytoplasm on light microscopy
[8]. SCC's show a strong and diffuse immunoreactivity for
CD 56 and 80% positivity for TTF-1 tumour markers
[10,11]. TTF-1 is positive in most cases of pulmonary
small cell carcinoma, but also shows positive staining
with many high-grade neuroendocrine carcinomas of
non-pulmonary origin. The importance of TTF-1 is to
exclude metastatic Merkel cell carcinoma, which is TTF-1
negative [11]. Due to the extent of disease in our case it
was not possible to assess dysplastic changes of the sur-
rounding mucosa. In the absence of a lung primary com-
bined with the immunohistochemical profile of the
appendiceal tumour suggests that this patient had a pure
extrapulmonary SCC of her appendix. Although carcinoid
tumours account for 32–35% of all appendiceal neo-
plasms, SCC's of the appendix are rarer with only one pre-
viously reported case by Rossi et al and this was mixed
with adenocarcinoma [12-14]. To the authors' knowledge
this is the first reported case of a pure small cell carcinoma
of the appendix. Further investigative modalities with CT
imaging and bronchoscopy are mandatory to exclude a
pulmonary origin [2]. Although this patient had a positive
family of pulmonary neoplasia, she was a non-smoker
with no respiratory symptomatology and had a normal
chest CT scan. Following consultation with the respiratory
department following surgery, no further investigation
was requested as oncological treatment was the priority.
Unfortunately clinical presentation of ESC carcinoma is
usually at an advanced stage due to the aggressive nature
of the disease. Therapeutic modalities are determined by
the location and extent of disease. Chemotherapy remains
the treatment of choice. The role of radiotherapy and sur-
High-power microscopic view of the small cell carcinoma showing hyperchromatic nuclei, nuclear moulding and clump-ing of the nuclear chromatinFigure 4
High-power microscopic view of the small cell carcinoma
showing hyperchromatic nuclei, nuclear moulding and clump-
ing of the nuclear chromatin.
Publish with BioMed Central and every
scientist can read your work free of charge
"BioMed Central will be the most significant development for
disseminating the results of biomedical research in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
World Journal of Surgical Oncology 2008, 6:4 http://www.wjso.com/content/6/1/4
Page 4 of 4
(page number not for citation purposes)
gical intervention remain limited, with surgery often only
being used for the treatment of localised disease [15].
Combination chemotherapy regimens using cisplatin-
etoposide are the most commonly used with response
rates of up to 70% [4]. There are no definite chemothera-
peutic regimens for ESC of the colon due to the small
patient numbers and clinically advanced disease at pres-
entation.
The prognosis for ESC is similar to pulmonary SCC's and
remains poor with a rapidly deteriorating clinical course.
Five-year survival is less than 13% [15]. The mean survival
for gastrointestinal ESC is less than 5-months with a 3-
and 8-month mean survival for extensive and localised
disease respectively [16].
Competing interests
The author(s) declare that they have no competing inter-
ests.
Authors' contributions
AOK: Involved in the literature review, manuscript prepa-
ration and manuscript editing. MEOD: Involved in the
conception of the report, literature review, manuscript
preparation, manuscript editing and manuscript submis-
sion. RS: Involved in the critical analysis of the histopa-
thology in the case report and manuscript review. PDC:
Involved in the manuscript editing and manuscript
review. JL: Involved in manuscript editing and manuscript
review.
All authors have read and approved the final manuscript.
Acknowledgements
The authors would like to acknowledge Dr Damian McManus for his assist-
ance in the production of the histopathological images.
Written informed patient consent was obtained from the patient for the
publication of this study.
This was presented at the Ulster Society of Gastroenterology, Belfast,
Northern Ireland – 18th October 2007.
References
1. Wu Z, Ma JY, Yang JJ, Zhao YF, Zhang SF: Primary small cell car-
cinoma of oesophagus: Report of 9 cases and review of liter-
ature. World J Gastroenterol 2004, 10:3680-3682.
2. Remick SC, Ruckdeschel JC: Extrapulmonary and pulmonary
small-cell carcinoma: tumor biology, therapy, and outcome.
Med Pediatr Oncol 1992, 20:89-99.
3. Kim HC, Park SI, Park SJ, Shin HC, Oh MH, Kim HH, Bae WK, Kim
IY: Small cell carcinoma of the colon: barium study and CT
findings. Br J Radiol 2005, 78:255-256.
4. Levenson RM Jr, Ihde DC, Matthews MJ, Cohen MH, Gazdar AF, Bunn
PA Jr, Minna JD: Small cell carcinoma presenting as an
extrapulmonary neoplasm: sites of origin and response to
chemotherapy. J Natl Cancer Inst 1981, 67:607-612.
5. Ohmura Y, Takiyama W, Mandai K, Doi T, Nishikawa Y: Small cell
carcinoma of the oesophagus: a case report. Jpn J Clin Oncol
1997, 27:95-100.
6. Demellawy DE, Samkari A, Sur M, Denardi F, Alowami S: Primary
small cell carcinoma of the cecum. Ann Diagn Pathol 2006,
10:162-165.
7. Kim JH, Lee SH, Park J, Kim HY, Lee SI, Nam EM, Park JO, Kim K, Jung
CW, Im YH, Kang WK, Lee MH, Park K: Extrapulmonary small-
cell carcinoma: A single-institution experience. Jpn J Clin Oncol
2004, 34:250-254.
8. Remick SC, Hafez GR, Carbone PP: Extrapulmonary small cell
carcinoma. A review of the literature with emphasis on ther-
apy and outcome. Medicine (Baltimore) 1987, 66:457-471.
9. Pearse AGE: The APUD cell concept and its implications in
pathology. Pathol Annu 1974, 9:27-41.
10. Kaufmann O, Georgi T, Dietel M: Utility of 123C3 monoclonal
antibody against CD56 (NCAM) for the diagnosis of small
cell carcinomas on paraffin sections. Hum Pathol 1997,
28:1373-1378.
11. Kaufmann O, Flath B, Splath-Schwalbe E, Possinger K, Dietel M:
Immunohistochemical detection of CD10 with monoclonal
antibody 56C56 on paraffin sections. Am J Clin Pathol 1999,
111:117-122.
12. Rossi G, Bertolini F, Sartori G, Bigiani N, Cavazza A, Foroni M, Valli
R, Rindi G, De Gaetani C, Luppi G: Primary mixed adenocarci-
noma and small cell carcinoma of the appendix: a clinico-
pathologic, immunohistochemical, and molecular study of a
hitherto unreported tumor. Am J Surg Pathol 2004,
28:1233-1239.
13. O'Donnell ME, Carson J, Garstin WIH: Surgical treatment of
malignant carcinoid tumours of the appendix. Int J Clin Pract
2007, 61:431-437.
14. O'Donnell ME, Badger SA, Beattie GC, Carson J, Garstin WIH:
Malignant neoplasms of the appendix. Int J Colorectal Dis 2007,
22:1239-1248.
15. Shamelian SO, Nortier JW: Extrapulmonary small-cell carci-
noma: report of three cases and update of therapy and prog-
nosis. Neth J Med 2000, 56:51-55.
16. Casas F, Ferrer F, Farr'us B, Casals J, Biete A: Primary small cell
carcinoma of the esophagus: A review of the literature with
emphasis on therapy and prognosis. Cancer 1997, 80:1366-72.


























%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)