BioMed Central
Page 1 of 4
(page number not for citation purposes)
World Journal of Surgical Oncology
Open Access
Case report
Surgical treatment of a rare primary renal carcinoid tumor with
liver metastasis
Roberto Gedaly*1, Hoonbae Jeon1, Thomas D Johnston1,
Patrick P McHugh1, Randall G Rowland2 and Dinesh Ranjan1
Address: 1Division of Transplantation and Hepatobiliary Surgery, Department of Surgery, University of Kentucky Medical Center, Lexington,
Kentucky, USA and 2Division of Urology, Department of Surgery, University of Kentucky Medical Center, Lexington, Kentucky, USA
Email: Roberto Gedaly* - rgeda2@uky.edu; Hoonbae Jeon - rgeda2@uky.edu; Thomas D Johnston - tdjohn1@uky.edu;
Patrick P McHugh - patrick.mchugh@uky.edu; Randall G Rowland - rrowlan@email.uky.edu; Dinesh Ranjan - dranj1@uky.edu
* Corresponding author
Abstract
Background: Carcinoid tumors are characteristically low grade malignant neoplasms with
neuroendocrine differentiation that arise in various body sites, most commonly the lung and
gastrointestinal tract, but less frequently the kidneys, breasts, ovaries, testes, prostate and other
locations. We report a case of a carcinoid of renal origin with synchronous single liver metastases
on radiological studies.
Case presentation: A 45 year-old patient who presented with abdominal pain was found on CT
scan to have lesions in the right ovary, right kidney, and left hepatic lobe. CA-125, CEA, and CA
19-9 were within normal limits, as were preoperative liver function tests and renal function. Biopsy
of the liver mass demonstrated metastatic neuroendocrine tumor. At laparotomy, the patient
underwent total abdominal hysterectomy with bilateral salpingo-oophorectomy, radical right
nephrectomy with lymphadenectomy, and left hepatectomy. Pathology evaluation reported a right
ovarian borderline serous tumor, well-differentiated neuroendocrine carcinoma of the kidney
(carcinoid) with 2 positive retroperitoneal lymph nodes, and a single liver metastasis.
Immunohistochemistry revealed that this lesion was positive for synaptophysin and CD56, but
negative for chromogranin as well as CD10, CD7, and CD20, consistent with a well-differentiated
neuroendocrine tumor. She is doing well one year after her initial surgery, with no evidence of
tumor recurrence.
Conclusion: Early surgical intervention, together with careful surveillance and follow-up, can
achieve successful long-term outcomes in patients with this rare malignancy.
Background
Neuroendocrine carcinomas may originate in a wide vari-
ety of tissues and organs, including those that do not nor-
mally contain neuroendocrine cells [1]. These tumors may
occur in pure forms or in association with conventional
adenocarcinomas or squamous cell carcinomas [2]. Neu-
roendocrine tumors of the kidney include carcinoids,
atypical carcinoids, and small cell carcinomas [2]. Intrare-
nal pheochromocytoma, neuroblastoma, and primitive
neuroectodermal tumors may also occur [3]. They may
Published: 22 April 2008
World Journal of Surgical Oncology 2008, 6:41 doi:10.1186/1477-7819-6-41
Received: 31 January 2008
Accepted: 22 April 2008
This article is available from: http://www.wjso.com/content/6/1/41
© 2008 Gedaly et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Surgical Oncology 2008, 6:41 http://www.wjso.com/content/6/1/41
Page 2 of 4
(page number not for citation purposes)
present clinically with gross hematuria or as a mass
detected on imaging studies. NE lesions of the kidney are
currently classified as well- or poorly-differentiated, both
being extremely uncommon [2,4]. Well-differentiated
neuroendocrine tumors of renal origin are usually carci-
noids, and fewer than 56 cases have been reported in the
literature [5]. There is an interesting, and as yet unex-
plained, association of renal carcinoids with horseshoe
kidneys [5-7]. The behavior of renal carinoids is not well
defined owing to the small number of reported cases, and
therefore prognoses are difficult to predict. Patients with
advanced disease have been reported to survive for long
periods of time even in the presence of tumor spread
[5,8]. Progression of hepatic metastases is the predomi-
nant cause of death in patients with gastrointestinal and
other cancers. For this reason the treatment of these
lesions has been the focus of multiple therapeutic
approaches. We report a case of a carcinoid from renal ori-
gin with a synchronous single liver metastasis on radio-
logical studies. We will discuss different aspects of this
unusual tumor, with emphasis on the treatment of liver
metastases.
Case presentation
We evaluated a 45 year-old patient who presented initially
with abdominal pain. Abdominal and pelvic CT scan
showed lesions in the right ovary, right kidney, and left
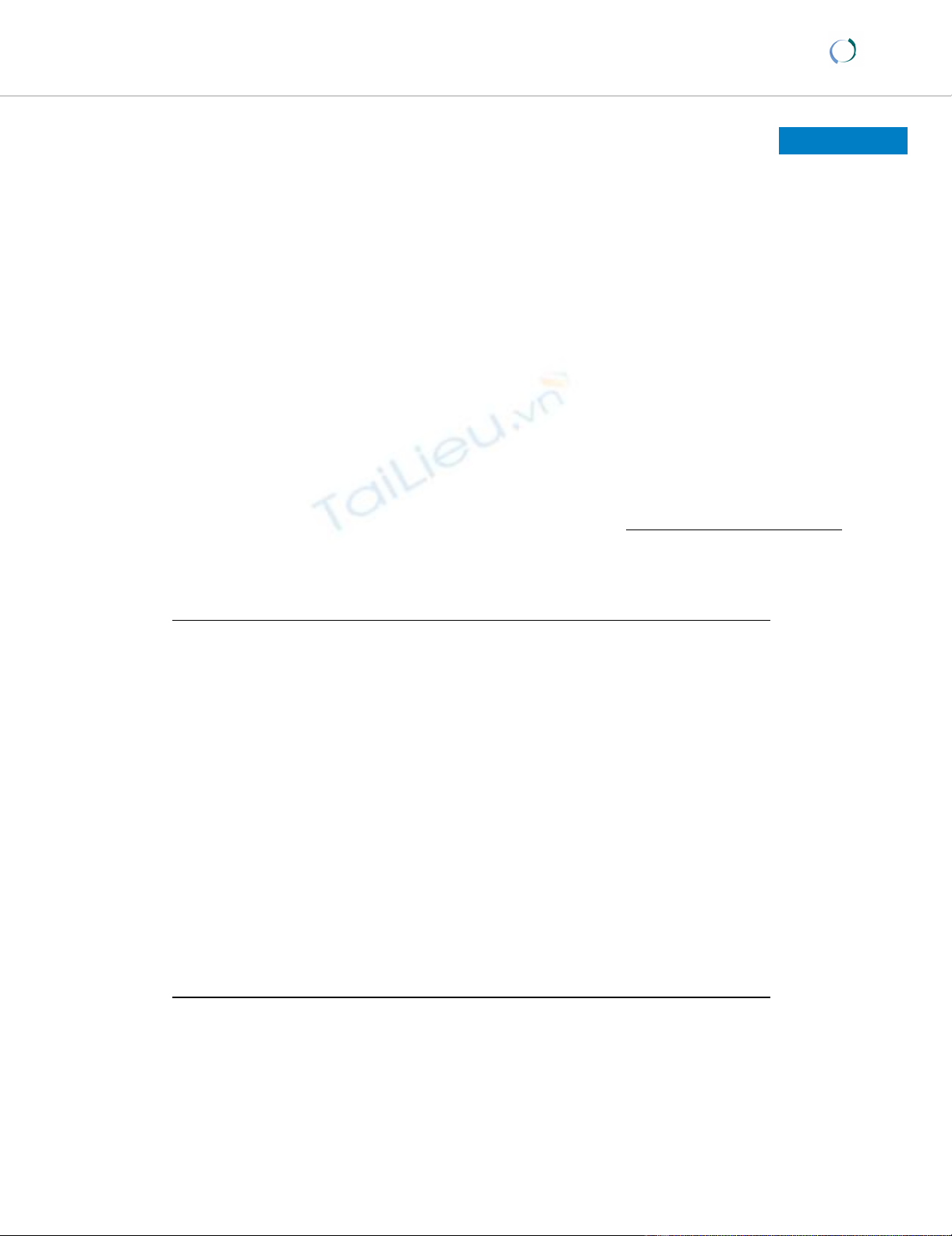
hepatic lobe. The right kidney mass was 8.0 cm in diame-
ter, with areas of calcification in the periphery of the
tumor inferiorly (Figure 1). In addition, there was one
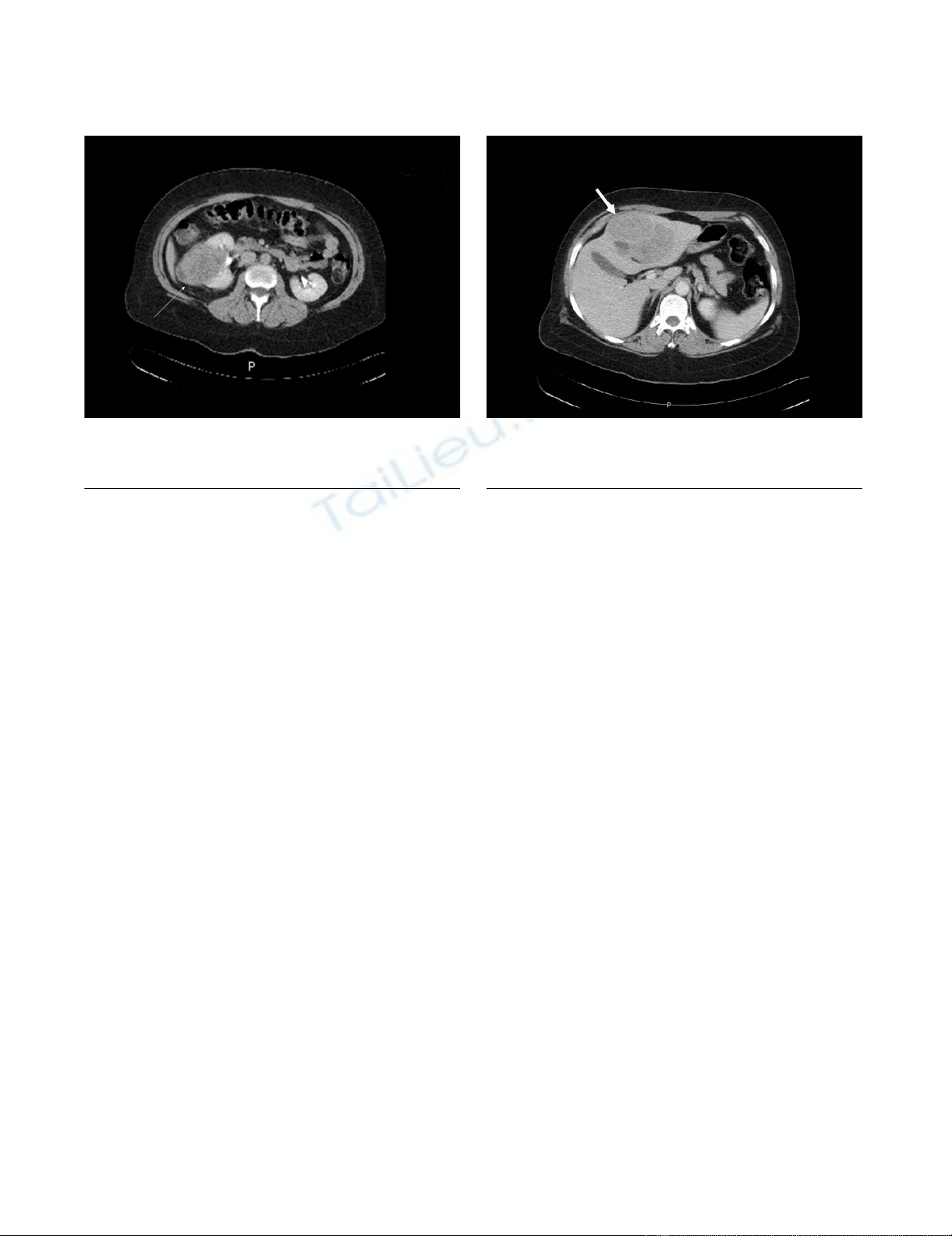
liver lesion, 9.7 cm in greatest diameter, located in seg-
ments 2 and 3 with extension into segment 4 of the left
lobe (Figure 2). The liver and kidney tumors showed sim-
ilar densities on CT scan. The right ovarian mass was mul-
tiloculated, measuring 8.7 cm in diameter. The uterus and
left ovary appeared normal. CT scan of the chest showed
no lesions. Tumor markers CA-125, CEA and CA 19-9
were within normal limits, as were preoperative liver func-
tion tests and renal function. A percutaneous biopsy of the
liver mass was performed, which the pathologist reported
to be metastatic neuroendocrine tumor. The patient was
subsequently taken to the operating room, where she
explored through a long midline incision; extensive
abdominal examination was performed and no perito-
neal seeding was found. The right ovary was removed first
and sent for frozen section. Pathology reported a border-
line tumor of the ovary; a total abdominal hysterectomy
with bilateral salpingo-oophorectomy was performed.
This was followed by a radical right nephrectomy with
lymphadenectomy and a formal left hepatectomy. Final
pathology reported a right ovarian borderline serous
tumor, well-differentiated neuroendocrine carcinoma of
the kidney (carcinoid) with 2 positive retroperitoneal
lymph nodes, and a single liver metastasis. Immunohisto-
chemistry revealed that this lesion was positive for synap-
tophysin and CD56, but negative for chromogranin as
well as CD10, CD7, and CD20. These features are consist-
ent with a well-differentiated neuroendocrine tumor. An
octreotide scan was performed 2 months after surgery,
which suggested the possibility of positive retroperitoneal
lymph nodes. The patient underwent a laparoscopic left
retroperitoneal para-aortic lymph node dissection, and 2
out of 5 lymph nodes were positive for tumor, with histo-
logic features similar to the original lesions. The patient is
doing well one year after her initial surgery, with no evi-
dence of tumor recurrence.
CT image showing the metastatic lesion in segments 2, 3 and 4 of the left hepatic lobeFigure 2
CT image showing the metastatic lesion in segments
2, 3 and 4 of the left hepatic lobe.
CT image showing the primary lesion in the right kidneyFigure 1
CT image showing the primary lesion in the right kid-
ney.

World Journal of Surgical Oncology 2008, 6:41 http://www.wjso.com/content/6/1/41
Page 3 of 4
(page number not for citation purposes)
Discussion
Carcinoid tumors are characteristically low grade malig-
nant neoplasms with neuroendocrine differentiation that
arise in various body sites, most commonly the lung and
gastrointestinal tract, but less frequently the kidneys,
breasts, ovaries, testes, prostate and other locations. The
prognosis of carcinoid tumors of renal origin is unclear
due to the rarity of these lesions. The pathogenesis of renal
carcinoid tumors (RCT) is controversial. Several hypothe-
ses support that RCT are derived from interspersed neu-
roendocrine cells associated with acquired and congenital
abnormalities such as metaplasia of pyelocaliceal urothe-
lium induced by chronic inflammation, misplaced or
entrapped neural crest or pancreatic tissue in the kidney
during embryogenesis, activation of gene sequences com-
mon to neuroendocrine programmed cells in multipotent
stem cells, or concurrent congenital abnormalities [9-12].
In 2006, an extensive review of the literature on primary
RCT was published by Romero et al. [5]. In this report, the
authors collected all previous reports by other centers for
a total of 56 cases. Renal carcinoids were associated with
another renal pathology in 26.8% of cases [5]. Only 7% of
these patients presented with carcinoid syndrome at the
time of diagnosis; interestingly, 4 other patients (7%) pre-
sented with symptoms related to other neuroendocrine
syndromes. The median patient age was 49 years, with a
range of 12 to 68 years. Calcifications were present on
26.5% of imaging studies. Median tumor size was 8.4 cm
(range 1.5 to 30 cm) with 73.6% of patients presenting
with tumors greater than 4 cm. Microscopically, 62.5% of
lesions showed a mixed growth pattern with 65% demon-
strating a predominant trabecular or ribbon-like growth
pattern. Mitotic figures were absent or rare in 83.3% of
reported cases. Immunohistochemistry demonstrated
many different patterns; nevertheless, most lesions were
positive for Grimelius, synaptophysin, neuron-specific
enolase and chromogranin but negative for Fontana-Mas-
son. Metastases were present in 50% of cases with para-
aortic and hilar lymph nodes being the most common
locations. Liver metastases occurred in 34% of cases.
Metastases to the bone and spleen were also described but
were much less common. Surgery was considered the
treatment of choice for RCT, and long-term survival was
achieved even in patients with lymph node metastases.
Tumor size smaller than 4 cm at the time of diagnosis and
lesions confined to the kidney were associated with a
lesser incidence of metastases and better prognosis [5].
Mitotic rate was also implicated as a prognostic patholog-
ical factor.
The octreotide scan is considered the most important
investigation for surveillance after resection. Following
chromogranin and 5-HIAA is also recommended, even in
the absence of symptoms. Additional neuroendocrine
markers can be tested if they were found to be positive
prior to surgery. CT and/or MRI can be used as imaging
studies for surveillance. New metastases have been
reported as long as 7 years after resection, indicating that
long term follow up is needed.
The treatment of liver metastases from RCT is not well
defined due to scarcity of cases. Most of the experience
regarding the treatment of metastatic neuroendocrine dis-
ease in the liver comes from those tumors originating in
the gastrointestinal tract, and in these cases, the mainstay
of treatment is resection [13-15]. In our patient, an aggres-
sive surgical approach including resection of the liver
metastasis was chosen based on the biopsy results demon-
strating a neuroendocrine tumor, the fact that the lesion
was solitary, and that an anatomic resection could be per-
formed to achieve negative margins. In the last few years
some authors have suggested that even in the presence of
extensive disease, liver resection for cytoreduction may be
not only palliative, but also may increase survival [16,17].
Nagorney et al. [16] have proposed that surgical resection
is indicated if the primary lesion is resectable or has been
resected, which makes 90% of liver metastases either
resectable or ablatable. An impressive 4-year survival rate
of 75% has been achieved with this approach. Interest-
ingly, they showed no survival difference between
patients undergoing complete versus incomplete resec-
tion. Other reports have showed that resection of neu-
roendocrine tumors may achieve 5-year survival rates in
the range of 47 to 92% [14,18,19], with resolution of
symptoms in more that 90% and very low operative mor-
tality.
Tumor recurrence has been a major problem after surgical
treatment. Resection, ablation, or both in combination
can be used to treat tumor recurrence [16]. Extensive int-
rahepatic recurrence can be treated with either emboliza-
tion or chemoembolization, since these are usually
hypervascular lesions. Systemic chemotherapy may be
used in the presence of extrahepatic spread of disease [20-
22]. Patients with pancreatic neuroendocrine tumors have
been more responsive to chemotherapy than carcinoids.
Since carcinoid lesions are low-grade, well-differentiated
tumors with a low proliferation index, they are less likely
to be responsive to chemotherapy. Somatostatin ana-
logues like octreotide and more recently lanreotide, which
can be given monthly, have been utilized to treat patients
with advanced disease. Response rate has been variable
and may correlate to octreotide scan, but stabilization of
disease has been seen in 36 to 70% of patients, with a
mean duration of 12 months [23]. Interferon alfa has also
been used in neuroendocrine tumors with low objective
response rate, but stabilization of the disease has been
observed in 40 to 60% of cases [16].
Publish with BioMed Central and every
scientist can read your work free of charge
"BioMed Central will be the most significant development for
disseminating the results of biomedical research in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
World Journal of Surgical Oncology 2008, 6:41 http://www.wjso.com/content/6/1/41
Page 4 of 4
(page number not for citation purposes)
Conclusion
Early surgical intervention, together with careful surveil-
lance and follow-up, can achieve successful long-term
outcomes in patients with this rare malignancy.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
RG and RGR conceived of the study; RG conducted litera-
ture review and prepared the draft manuscript; RG, HJ,
TDJ, PPM, and RGR performed critical editing of content
and helped in preparation of the manuscript; RG and DR
edited the final version. All authors read and approved of
the final version of the manuscript
Acknowledgements
Written informed consent was obtained from the patient for publication of
this case report.
References
1. Zuetenhorst JM, Taal BG: Metastatic carcinoid tumors: a clinical
review. Oncologist 2005, 10:123-131.
2. Osamura RY, Chie I, Kajiwara H, DeLellis RA: Neuroendocrine
carcinomas of diverse sites. Pathology Case Reviews 2006,
11:282-291.
3. Parham DM, Roloson GJ, Feely M, Green DM, Bridge JA, Beckwith JB:
Primary malignant neuroepithelial tumors of the kidney: a
clinicopathologic analysis of 146 adult and pediatric cases
from the National Wilms' Tumor Study Group Pathology
Center. Am J Surg Pathol 2001, 25:133-146.
4. Kurl S, Rytkonen H, Farin P, Ala-Opas M, Soimakallio S: A primary
carcinoid tumor of the kidney: a case report and review of
the literature. Abdom Imaging 1996, 21:464-467.
5. Romero FR, Rais-Bahrami S, Permpongkosol S, Fine SW, Kohanim S,
Jarrett TW: Primary carcinoid tumors of the kidney. J Urol
2006, 176:2359-2366.
6. Rodriguez-Covarrubias F, Gomez X, Valerio JC, Lome-Maldonado C,
Gabilondo F: Carcinoid tumor arising in a horseshoe kidney.
Int Urol Nephrol 2006.
7. Isobe H, Takashima H, Higashi N, Murakami Y, Fujita K, Hanazawa K,
Fujime M, Matsumoto T: Primary carcinoid tumor in a horse-
shoe kidney. Int J Urol 2000, 7:184-188.
8. McCaffrey JA, Reuter VV, Herr HW, Macapinlac HA, Russo P, Motzer
RJ: Carcinoid tumor of the kidney. The use of somatostatin
receptor scintigraphy in diagnosis and management. Urol
Oncol 2000, 5:108-111.
9. Begin LR, Guy L, Jacobson SA, Aprikian AG: Renal carcinoid and
horseshoe kidney: a frequent association of two rare entities
– a case report and review of the literature. J Surg Oncol 1998,
68:113-119.
10. Yoo J, Park S, Jung Lee H, Jin Kang S, Kee Kim B: Primary carcinoid
tumor arising in a mature teratoma of the kidney: a case
report and review of the literature. Arch Pathol Lab Med 2002,
126:979-981.
11. Schlussel RN, Kirschenbaum AM, Levine A, Unger P: Primary renal
carcinoid tumor. Urology 1993, 41:295-297.
12. Muthuphei MN: Primary renal carcinoid: report of a case. Cent
Afr J Med 1999, 45:327-329.
13. Chen H, Hardacre JM, Uzar A, Cameron JL, Choti MA: Isolated liver
metastases from neuroendocrine tumors: does resection
prolong survival? J Am Coll Surg 1998, 187:88-92. discussion 92–83.
14. Grazi GL, Cescon M, Pierangeli F, Ercolani G, Gardini A, Cavallari A,
Mazziotti A: Highly aggressive policy of hepatic resections for
neuroendocrine liver metastases. Hepatogastroenterology 2000,
47:481-486.
15. Sarmiento JM, Heywood G, Rubin J, Ilstrup DM, Nagorney DM, Que
FG: Surgical treatment of neuroendocrine metastases to the
liver: a plea for resection to increase survival. J Am Coll Surg
2003, 197:29-37.
16. DM Nagorney TDA, Que FG: Hepatic metastases from primary
neuroendocrine tumors. In Surgery of the Liver Biliary Tract and Pan-
creas Blumgart LH: Saunders; 2007:1195-1217.
17. Musunuru S, Chen H, Rajpal S, Stephani N, McDermott JC, Holen K,
Rikkers LF, Weber SM: Metastatic neuroendocrine hepatic
tumors: resection improves survival. Arch Surg 2006,
141:1000-1004. discussion 1005.
18. Nave H, Mossinger E, Feist H, Lang H, Raab H: Surgery as primary
treatment in patients with liver metastases from carcinoid
tumors: a retrospective, unicentric study over 13 years. Sur-
gery 2001, 129:170-175.
19. Norton JA, Warren RS, Kelly MG, Zuraek MB, Jensen RT: Aggres-
sive surgery for metastatic liver neuroendocrine tumors.
Surgery 2003, 134:1057-1063. discussion 1063–1055.
20. Kaltsas G, Mukherjee JJ, Plowman PN, Grossman AB: The role of
chemotherapy in the nonsurgical management of malignant
neuroendocrine tumours. Clin Endocrinol (Oxf) 2001, 55:575-587.
21. Oberg K: Diagnosis and treatment of carcinoid tumors. Expert
Rev Anticancer Ther 2003, 3:863-877.
22. Rivera E, Ajani JA: Doxorubicin, streptozocin, and 5-fluorour-
acil chemotherapy for patients with metastatic islet-cell car-
cinoma. Am J Clin Oncol 1998, 21:36-38.
23. Oberg K, Astrup L, Eriksson B, Falkmer SE, Falkmer UG, Gustafsen J,
Haglund C, Knigge U, Vatn MH, Valimaki M: Guidelines for the
management of gastroenteropancreatic neuroendocrine
tumours (including bronchopulmonary and thymic neo-
plasms). Part II-specific NE tumour types. Acta Oncol 2004,
43:626-636.


























%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)