BioMed Central
Page 1 of 4
(page number not for citation purposes)
Journal of Medical Case Reports
Open Access
Case report
Accelerated tibial fracture union in the third trimester of
pregnancy: a case report
Mudussar A Ahmad*, Damayanthi Kuhanendran, Irvine W Kamande and
Charalambos Charalambides
Address: Department of Trauma & Orthopaedics, The Whittington University Hospital, London, UK
Email: Mudussar A Ahmad* - mudussarahmad@hotmail.com; Damayanthi Kuhanendran - damy007@hotmail.com;
Irvine W Kamande - Irvinekamande@hotmail.com; Charalambos Charalambides - charalambos.charalambides@whittington.nhs.uk
* Corresponding author
Abstract
Introduction: We present a case of accelerated tibial fracture union in the third trimester of
pregnancy. This is of particular relevance to orthopaedic surgeons, who must be made aware of
the potentially accelerated healing response in pregnancy and the requirement for prompt
treatment.
Case presentation: A 40 year old woman at 34 weeks gestational age sustained a displaced
fracture of the tibial shaft. This was initially treated conservatively in plaster with view to intra-
medullary nailing postpartum. Following an emergency caesarean section, the patient was able to
fully weight bear without pain 4 weeks post injury, indicating clinical union. Radiographs
demonstrated radiological union with good alignment and abundant callus formation. Fracture
union occurred within 4 weeks, less than half the time expected for a conservatively treated tibial
shaft fracture.
Conclusion: Long bone fractures in pregnancy require clear and precise management plans as
fracture healing is potentially accelerated. Non-operative treatment is advisable provided
satisfactory alignment of the fracture is achieved.
Introduction
Tibial fractures are the second most common long bone
fracture. Treatment varies according to fracture displace-
ment, complexity and whether the fracture is open or
closed. The options are non-operative treatment, with
plaster immobilization and traction, or operative treat-
ment, with intra-medullary nailing, plating and external
fixation. The potential complications of non-operative
treatment include delayed union, mal-union and non-
union. Operative management has similar complications
with the addition of wound infection, osteomyelitis and
fat embolism.
Surgical intervention in pregnancy presents a risk to the
foetus. However surgery can be successfully performed
when a multidisciplinary team approach is used [1].
Fracture healing occurs in three phases: inflammatory,
reparative and remodelling [2]. This is a dynamic process
which is mainly regulated by local interactions among
cells and tissues around the fracture site. Tissue repair is
Published: 9 February 2008
Journal of Medical Case Reports 2008, 2:44 doi:10.1186/1752-1947-2-44
Received: 9 November 2007
Accepted: 9 February 2008
This article is available from: http://www.jmedicalcasereports.com/content/2/1/44
© 2008 Ahmad et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Case Reports 2008, 2:44 http://www.jmedicalcasereports.com/content/2/1/44
Page 2 of 4
(page number not for citation purposes)
also influenced by hormones that act systemically, such as
insulin and glucocorticoid, and gonadal hormones, such
as oestrogen and androgens [3], which are all increased in
pregnancy.
Accelerated union of fractures has been seen in children
and in patients with head injuries, neurological disease
(e.g. spina bifida, paraplegia) and burns.
We present a case of accelerated tibial fracture union in a
pregnant woman.
Case presentation
A 40 year old obese African woman (weight 135 kg) who
was 34 weeks pregnant injured her right leg following a
fall in the bathroom. Previous medical history included
thalassaemia trait and severe bipolar affective disorder
which was being treated with Lithium Carbonate and
prochlorperazine. She was a non-smoker and did not
drink alcohol. On examination the leg was swollen,
slightly deformed with the skin intact and there was no
neurovascular deficit or evidence of compartment syn-
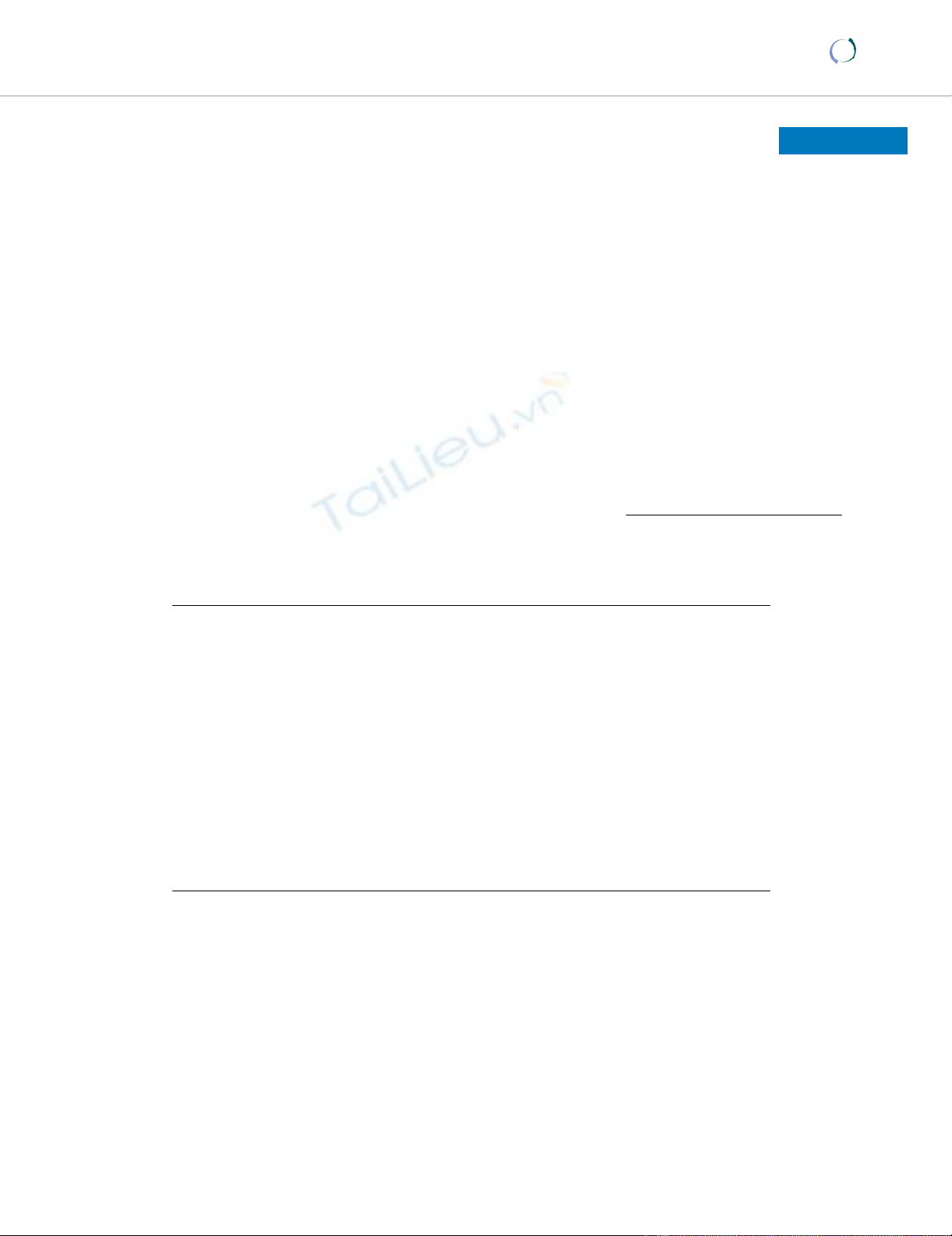
drome. Radiographs of the tibia revealed a displaced
oblique mid-shaft fracture of the right tibia, 42-A2.1 using
the AO classification (fig. 1).
The initial plan was non-operative treatment until post-
partum, after which the fracture would be stabilised by an
intra-medullary nail. She was admitted to hospital and a
below knee backslab followed by a full Sarmiento cast
applied. An above knee plaster could not be applied due
to thigh bulk. The patient was allowed to touch weight
bear for nursing purposes. Our main concern regarding
the non-operative management in a plaster cast was the
increased risk of developing a deep vein thrombosis. At 38
weeks of pregnancy, an emergency caesarean section was
performed and a healthy baby delivered.
Prior to the planned surgery in the post-natal period, it
was noticed that the patient was able to mobilise with full
weight bearing through the plaster without pain. Clinical
examination revealed no pain or movement at the fracture
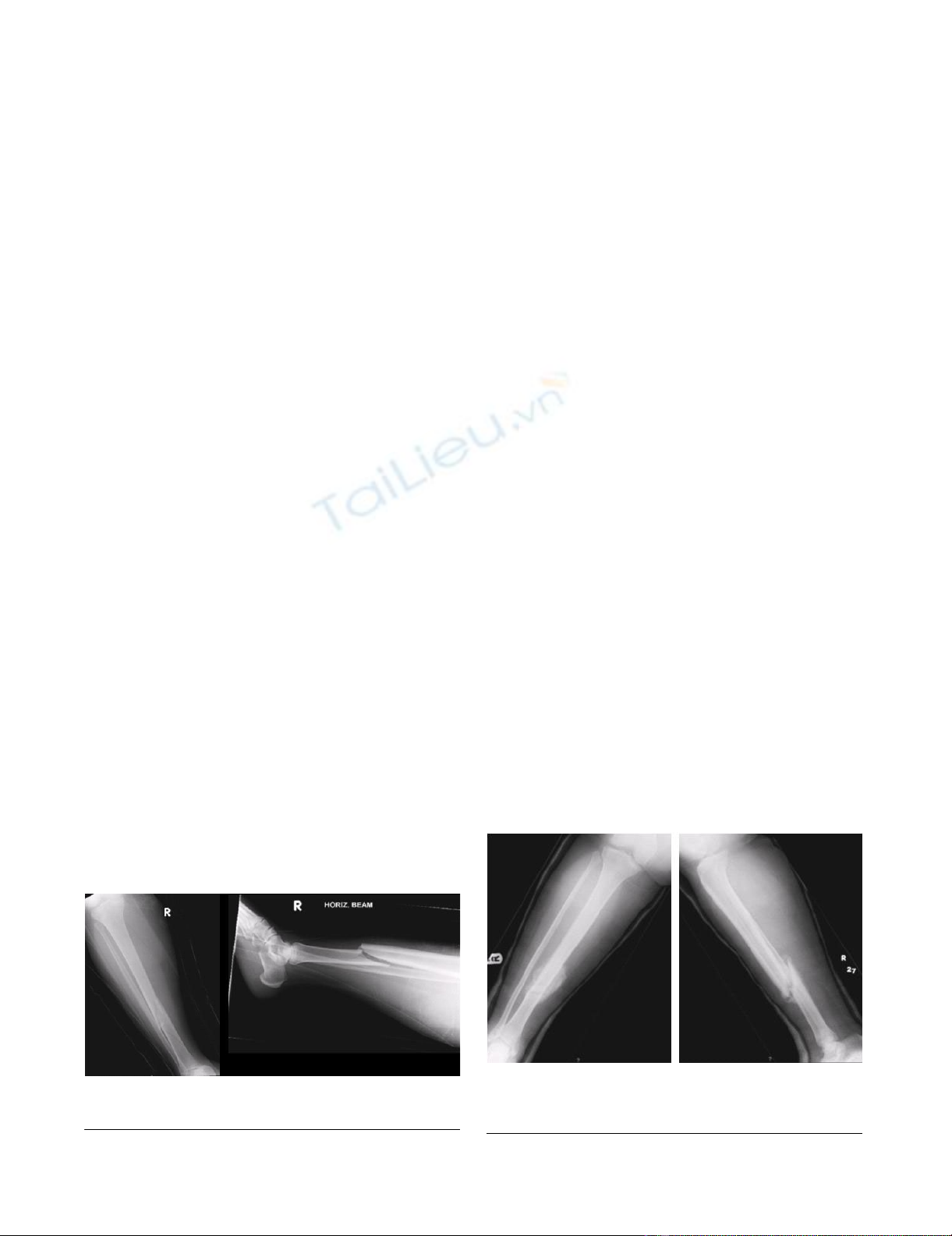
site indicating clinical union. Radiographs at four weeks
(fig. 2) showed satisfactory alignment and significant cal-
lus bridging all four cortices indicating radiological
union. The patient was allowed to fully mobilise as toler-
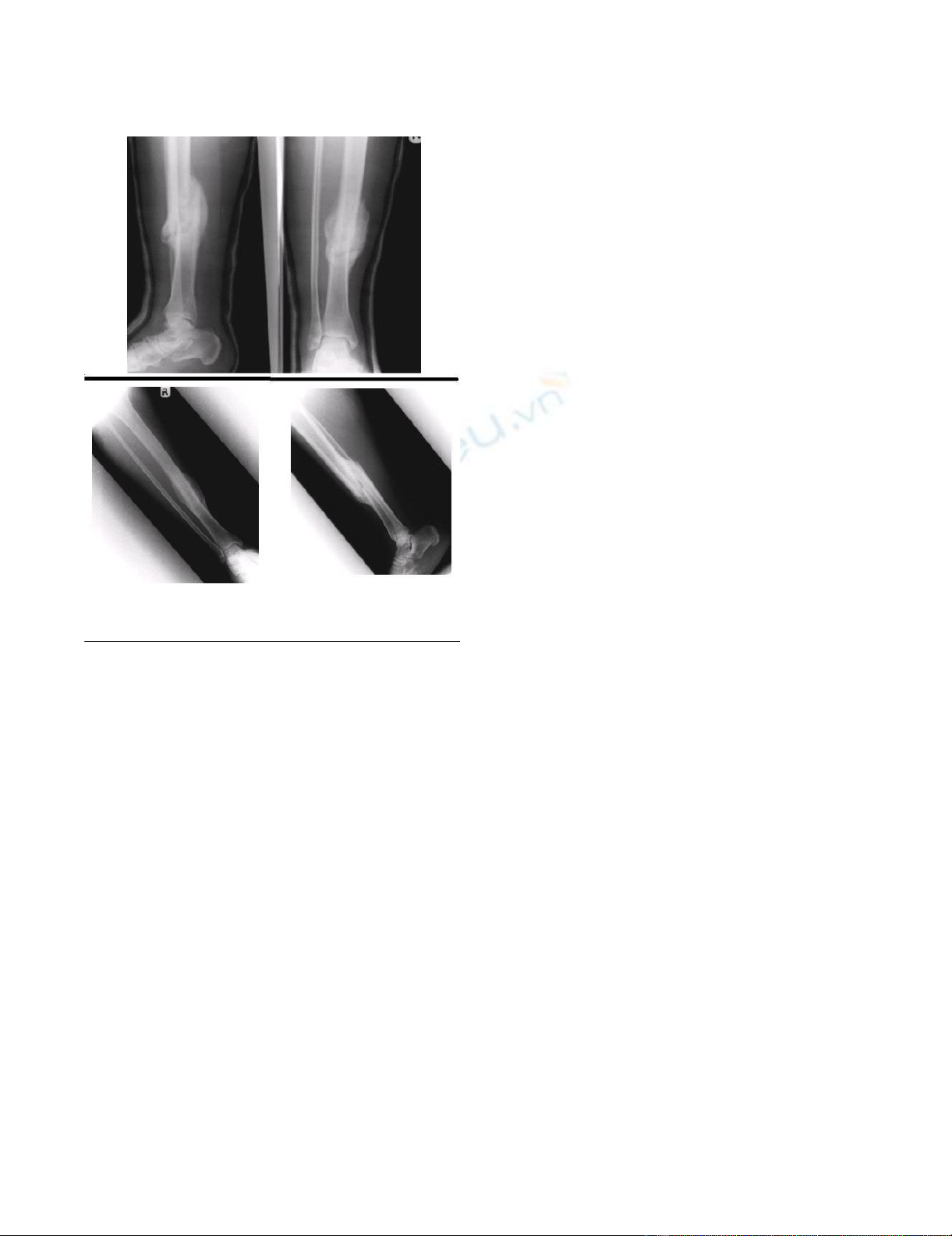
ated in an air cast boot and reviewed in four weeks with a
further radiograph that showed a consolidated fully
healed fracture (fig. 3).
Review two years post injury showed a united fracture (fig.
3). The patient was asymptomatic with no clinical
deformity and a full range of pain free motion in her ankle
and knee.
Discussion
Fracture healing is influenced by factors related to the
injury and those related to the patient. Factors related to
the injury include whether the fracture is open or closed,
the severity of soft tissue injury, the degree of contamina-
tion in cases of open fracture and the adequacy of reduc-
tion. Patient factors include age, smoking, alcohol intake
and the use of medications such as steroids or non-steroi-
dal anti-inflammatory drugs.
In this case, we propose that the main contributing factor
for accelerated union by four weeks is most likely hormo-
nal. In pregnancy, there is an increase in the level of ster-
oid hormones, initially with progesterone in the first
trimester followed by the oestrogens and prolactin in the
2nd and 3rd trimesters [4]. Oestrogen has well-documented
effects on bone formation and remodelling during frac-
ture healing [5]. Radioligand binding studies in a fibula
osteotomy (created fracture) model of fracture healing in
New Zealand rabbits demonstrated the presence of oes-
trogen receptors in fracture sites in a bimodal distribution
with a peak occurring on day 16 post-osteotomy [6]. Oes-
Radiograph following caesarean section, 4 weeks post injuryFigure 2
Radiograph following caesarean section, 4 weeks post
injury.
Initial radiographsFigure 1
Initial radiographs.
Journal of Medical Case Reports 2008, 2:44 http://www.jmedicalcasereports.com/content/2/1/44
Page 3 of 4
(page number not for citation purposes)
trogen receptors have been shown to be present in fracture
callus [7]. It has also been shown that treating ovariect-
omized rats with oestrogen during fracture healing
strengthens the healing callus and increases expression of
cartilage matrix proteins [8]. This suggests high levels of
oestrogen at this specific time post fracture would have a
maximal effect on bone healing as the oestrogen receptors
in callus are also maximal at this stage. The hyperdynamic
circulation in pregnancy may also contribute to acceler-
ated fracture healing by delivering the cellular factors and
hormones to the fracture site at a faster rate. A significant
increase in heart rate can be demonstrated as early as the
5th week in pregnancy and this contributes to an increase
in cardiac output at this time [9]. There is a progressive
augmentation of stroke volume (10–20 ml) during the
first half of pregnancy, probably related to incremental
changes in plasma volume and as a consequence cardiac
output increases from an average of under 5 l/min before
pregnancy to approximately 7 l/min at the 20th week of
pregnancy [9]. This results in a faster delivery of cellular
factors and hormones to the fracture site.
This woman probably mobilised with full weight bearing
as comfort allowed in the plaster cast, as touch weight
bearing would have been unrealistic for someone weigh-
ing 135 kg. Early weight bearing has been shown to pro-
mote fracture healing and this may also have contributed
to accelerated fracture union. Kenwright et al compared
two groups of rigidly fixed tibial shaft fractures, one with
no movement and one with axial micromovement at the
fracture site (induced by weight bearing). Time to clinical
union and full weight bearing was significantly less and
fracture stiffness was greater in the micromovement group
[10].
Tibial fractures are a complex group of injuries with many
potential complications. A meta-analysis of published
studies between 1966 and 1993 of three methods of treat-
ment determining the clinical outcomes of the treatment
of closed tibial shaft fractures with immobilization in a
cast, open reduction with internal fixation or fixation with
an intra-medullary nail revealed open reduction and
internal fixation to be associated with a higher rate of
bony union by twenty weeks than treatment with a cast
[11].
In a prospective review of 13 studies which looked at 895
tibial shaft fractures treated by application of a plaster
cast, fixation with plate and screws, and reamed or
unreamed intra-medullary nailing, the combined inci-
dence of delayed and non-union was higher with closed
treatment (17.2%) in comparison to operative treatment
(2.6% with plate fixation, 8.0% with reamed nailing and
16.7% with unreamed nailing) [12]. These studies suggest
tibial fractures treated conservatively take longer to unite,
and should usually do so by approximately 20 weeks, 12
weeks longer than in our patient.
Conclusion
1. Long bone fractures in pregnancy require clear and pre-
cise management plans as fracture healing is potentially
accelerated.
2. Non-operative treatment is advisable provided satisfac-
tory alignment of the fracture in plaster is achieved early
on.
3. If operative treatment is delayed, technical difficulties
may be encountered during definitive surgery, due to the
potentially accelerated healing response.
4. A better understanding of the biology of bone healing
is required especially in pregnancy.
Competing interests
The author(s) declare that they have no competing inter-
ests.
Radiograph 8 weeks and 2 years post injuryFigure 3
Radiograph 8 weeks and 2 years post injury.
Publish with BioMed Central and every
scientist can read your work free of charge
"BioMed Central will be the most significant development for
disseminating the results of biomedical research in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
Journal of Medical Case Reports 2008, 2:44 http://www.jmedicalcasereports.com/content/2/1/44
Page 4 of 4
(page number not for citation purposes)
Authors' contributions
MAA analysed the literature, results, radiographs, wrote &
corrected the manuscript. DK did the literature search and
compiled results. IWK compiled the radiographs and
thought of the idea. CC corrected the draft of the manu-
script and approved for publication. All authors read and
approved the final manuscript.
Consent
Written informed consent was obtained from the patient
for publication of this case report and all accompanying
images. A copy of the written consent is available for
review by the Editor-in-Chief of this journal.
Acknowledgements
The patient on whom this case report is based.
References
1. Kloen P, Flik K, Helfet DL: Case report. Operative treatment of
acetabular fracture during pregnancy: a case report. Arch Orthop Trauma
Surg 2005, 125(3):209-12.
2. Wilkins KE: Article. Principles of fracture remodelling in chil-
dren. Injury, Int J Care Injured 2005, 36:S-A3-S-A11.
3. Kagel EM, Majeska RJ, Einhorn TA: Article. Effects of diabetes and
steroids on fracture healing. Curr Opin Orthop 1995, 6(5):7-13.
4. Johnson MH, Everitt BJ: Essential reproduction. 5th edition.
Blackwell Science; 2000:196-197.
5. Burnett CC, Reddi AH: Article. Influence of estrogen and pro-
gesterone on matrix-induced endochondral bone formation.
Calcif Tissue Int 1983, 35:609.
6. Monaghan BA, Kaplan FS, Lyttle DR, Fallon MD, Boden SD, Haddad
JG: Paper. Estrogen receptors in fracture healing. Clin Orthop
1992, 280:277-280.
7. Braidman IP, Hainey L, Batra G, Selby Pl, Saunders PT, Hoyland JA:
Article. Localisation of estrogen receptor beta protein
expression in adult human bone. J Bone Miner Res 2001,
16:214-220.
8. Bolander ME, Sabbagh R, Jeng C, Vivianno D, Boden SD: Paper.
Estrogen treatment during fracture repair strengthens heal-
ing callus in an osteoporotic model. Trans Orthop Res Soc 1992,
17:138.
9. Campbell S, Lees C: Physiological changes in pregnancy. Arnold
Seventeenth edition. 2000:48-49.
10. Kenwright J, Richardson JB, Goodship AE, Evans M, Kelly DJ, Spriggins
AJ, Newman JH, Burrough SJ, Harris JD, Rowley DI: Effect of con-
trolled axial micromovement on healing of tibial fracutres.
Lancet 1986, 22:1185-1187.
11. Littenberg B, Weinstein LP, McCarren M, Mead T, Swiontkowski MF,
Rudicel SA, Heck D: Review article. Closed fractures of the tib-
ial shaft. A meta-analysis of three methods of treatment. J
Bone Joint Surg Am 1998, 80:174-183.
12. Coles CP, Gross M: Review article. Closed tibial shaft frac-
tures: management and treatment complications. A review
of the prospective literature. Can J Surg 2000, 43:256-262.


![Báo cáo seminar chuyên ngành Công nghệ hóa học và thực phẩm [Mới nhất]](https://cdn.tailieu.vn/images/document/thumbnail/2025/20250711/hienkelvinzoi@gmail.com/135x160/47051752458701.jpg)























%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)