BioMed Central
Page 1 of 5
(page number not for citation purposes)
Journal of Medical Case Reports
Open Access
Case report
Acute disseminated encephalomyelitis mimicking late CNS relapse
of acute lymphoblastic leukaemia: case report
Ram Kumar*1, Shobha Nijalingappa1, John Grainger2 and Omar Ismayl1
Address: 1Department of Paediatric Neurology, Royal Manchester Children's Hospital, Hospital Road, Manchester, UK and 2Department of
Paediatric Haematology and Oncology, Royal Manchester Children's Hospital, Hospital Road, Manchester, UK
Email: Ram Kumar* - kumarr1@doctors.org.uk; Shobha Nijalingappa - drshobha77@yahoo.com; John Grainger - john.grainger@cmmc.nhs.uk;
Omar Ismayl - oismayl@doctors.org.uk
* Corresponding author
Abstract
Background: Acute encephalomyelopathy occurring after an allogeneic bone marrow transplant
for leukaemia is a diagnostic emergency. The diagnosis can be challenging since there is a wide set
of alternative diagnoses, including opportunistic infections and relapse of the leukaemia.
Case presentation: A 13-year old girl presented with a severe acute myelopathy and
encephalopathy. She was in prolonged remission from a central nervous system and bone marrow
relapse of an acute lymphoblastic leukaemia, treated with allogeneic bone marrow transplantation.
Neuroimaging showed multifocal grey and white matter lesions of demyelinating appearance in the
brain and entire spine. Immunophenotyping and cytogenetic investigations of the girl's
cerebrospinal fluid lymphocytosis excluded a late central nervous system relapse of her leukaemia.
The diagnosis was acute disseminated encephalomyelitis. With standard immunosuppressive
therapy, the girl had early cerebral recovery but a prolonged period of recovery from her
myelopathy.
Conclusion: Acute disseminated encephalomyelitis should be considered in the differential
diagnosis of acute encephalomyelopathy after bone marrow transplantation for leukaemia.
Demyelinating syndromes such as acute disseminated encephalomyelitis may be late sequelae of
bone marrow transplantation.
Background
Acute encephalomyelopathy occurring after bone marrow
transplantation for leukaemia is a diagnostic emergency.
The diagnosis is challenging since the differential is wide,
including opportunistic infections and leukaemia recur-
rence [1]. Acute disseminated encephalomyelitis (ADEM)
is an uncommon idiopathic immune-mediated demyeli-
nating disorder, recognised as a cause of encephalomy-
elopathy in previously well children [2]. We report a child
with acute disseminated encephalomyelitis occurring late
after successful allogeneic bone marrow transplantation
for an acute leukaemia whose presentation mimicked a
previous CNS leukaemic relapse.
Case presentation
A 13-year old girl presented with a rapidly progressive
paralysis and encephalopathy. She had a mild viral-like
illness for the preceding week, with lethargy. Over the
days preceding presentation she developed back pain and
difficulty in walking. On the morning of admission, she
Published: 9 February 2007
Journal of Medical Case Reports 2007, 1:4 doi:10.1186/1752-1947-1-4
Received: 22 January 2007
Accepted: 9 February 2007
This article is available from: http://www.jmedicalcasereports.com/content/1/1/4
© 2007 Kumar et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Case Reports 2007, 1:4 http://www.jmedicalcasereports.com/content/1/1/4
Page 2 of 5
(page number not for citation purposes)
developed a headache, vomiting, a fluctuating level of
consciousness and became unable to move her limbs.
Neurological examination showed an encephalopathic
girl, with four limb paralysis, absent deep tendon and
abdominal reflexes, and mild bilateral facial weakness. A
high thoracic (C4) sensory level, severe urinary retention
and stool incontinence was evident. Systemic examina-
tion did not reveal pyrexia, rash, lymphadenopathy,
hepatosplenomegaly or sepsis.
Her remote clinical history was notable: at age 2 years, she
had developed acute lymphoblastic leukaemia (ALL),
common B-cell variant. Six months after completing
chemotherapy using the UKALLXI protocol, the girl re-
presented with an encephalopathy due to a CNS and bone
marrow relapse of the leukaemia. The girl received cranial
irradiation and further chemotherapy on the MRC UKALL
R2 relapse protocol which achieved a further remission.
Because of the high risk of further relapses, she proceeded
to have an bone marrow transplant (BMT) with a matched
unrelated male donor. Total body irradiation was used in
conditioning for the BMT. Following the BMT, the girl was
in prolonged remission for the following 7 years with no
overt CNS or systemic sequelae.
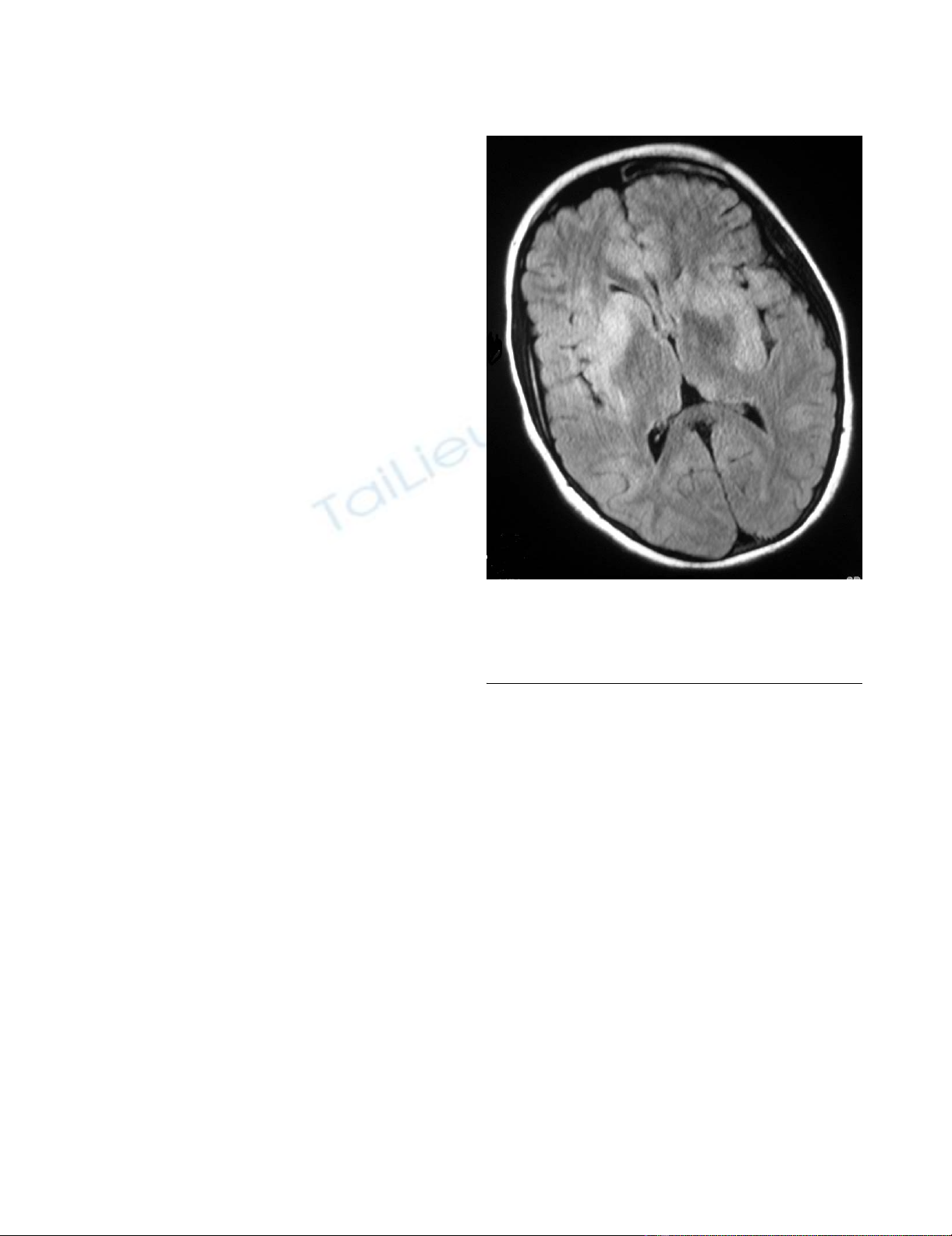
Initial MR imaging showed diffuse involvement of the
CNS (Figures 1 and 2). The spinal cord was diffusely swol-
len showing central cord T2 hyperintensity from C1 to the
conus. There were multifocal grey and white matter
lesions in the cerebral cortex, subcortical areas and cere-
bellum which showed diffuse gadolinium enhancement.
The appearances were consistent with an infective or
inflammatory encephalomyelitis, but the girl's remote
history and presentation raised the concern of a recurrent
CNS relapse of ALL.
CSF examination revealed 125 white cells with a lym-
phoblastic appearance and 5 red cells. CSF protein (0.61
g/l) and CSF:blood lactate ratio (3.2:1.2 mmol/l) were
raised with a low CSF: glucose ratio (4.3:8.9 mmol/l). CSF
cytospin showed increased proportion of lymphocytes
which further increased suspicion of ALL relapse (Figure
3). Immunophenotyping of the CSF cells demonstrated
the cells were CD10 negative, strongly CD2 and CD7 pos-
itive and terminal deoxynucleotidyl transferase (TdT) neg-
ative. These findings suggested that the cells were mature
T-cells. Cytogenetic studies and FISH using centromeric X
and Y-chromosome markers on the CSF lymphocytes con-
firmed that the overwhelming majority of cells were of
male donor type (6–14% of cells were of host origin but
not clonal). These CSF findings, along with a normal
peripheral blood count and normal bone marrow biopsy
confirmed that the girl's illness was not due relapse of her
previous ALL.
The girl was treated with intravenous high-dose methyl-
prednisolone and aciclovir. Blood-brain barrier studies
showed an abnormal CSF IgG index; oligoclonal bands
were not detected. Further negative tests included: CSF
culture; CSF PCR for HSV1 and 2, VZV, EBV, HHV6/7,
adenovirus, echovirus, parechovirus, enterovirus and
echovirus; serology for influenza, mycoplasma, Chlamy-
dia, and toxoplasma; ASOT, ANA, ANCA, anticardiolipin
antibodies, tissue autoantibodies. Immune function tests
did not reveal an underlying inmmunosuppression. A
presumptive diagnosis of ADEM with associated trans-
verse myelitis was made.
The girl's encephalopathy resolved over succeeding days
without overt cerebral sequelae, but spinal recovery was
much slower. A repeat MRI at 2 weeks after onset showed
resolving brain and spinal lesions. Her disability slowly
improved over several months: Barthel activities of daily
living index was 15/100 at 3 weeks, 40/100 at 7 weeks,
and 85/100 at discharge from hospital 3 months after
onset. At last review, 10 months after onset, her Barthel
index was 100/100. She was mobile on her feet without
aids, and had just ceased intermittent catheterisation for
Axial FLAIR sequence magnetic resonance image of brain at admissionFigure 1
Axial FLAIR sequence magnetic resonance image of
brain at admission. There are hyperintense multifocal
lesions in the deep grey nuclei, subcortical white matter and
cortex.

Journal of Medical Case Reports 2007, 1:4 http://www.jmedicalcasereports.com/content/1/1/4
Page 3 of 5
(page number not for citation purposes)
urine voiding. She was unable to walk on her heels, and
had lingering fatiguability.
Discussion
This girl presented with the features of a severe acute
encephalomyelopathy. We made the diagnosis of ADEM
based on her MR imaging and exclusion of competing
diagnoses. Being a diagnosis of exclusion, a discussion of
ADEM entails discussion of the differential diagnosis
(Table 1).
An isolated CNS relapse of acute leukaemia was the initial
concern because of the girl's previous CNS relapse. Con-
cern was heightened by her marked CSF lymphocytosis.
Isolated CNS relapse of leukaemia is uncommon after
BMT in prolonged remission [3]. The MRI appearance that
would be expected in CNS relapse of leukaemia is menin-
gitic contrast enhancement due to leukaemic infiltrates,
rather than the non-space occupying parenchymal lesions
of the brain and intramedullary spine seen in this girl [4].
We demonstrated that the girl did not have a CNS relapse
of her original common variant ALL using immunophe-
notyping and cytogenetics. Immunophenotyping, using
fluorescent monoclonal antibodies, showed that the CSF
cells lacked the CD10 antigen – a marker of immature
common lineage lymphocytes which would be expected
to be positive in a relapse. The cells demonstrated the CD2
and CD7 antigens which are both markers of T-cells. The
absence of TdT, a marker of immature lymphocytes,
showed the T-cells were mature reactive cells rather than
lymphoblasts. The cytogenetic testing showed that the
cells were not clonal, whereas clonal expansion would be
expected in a relapse. Cytogenetic testing also showed the
cells were derived mainly from the girl's male BMT donor,
CSF cytospin (x50 magnification)Figure 3
CSF cytospin (x50 magnification). CSF cytospin with
Giemsa's stain showing pronounced lymphocytosis.
Sagittal T2-weighted magnetic resonance image of spine at admissionFigure 2
Sagittal T2-weighted magnetic resonance image of
spine at admission. There is longitudinal hyperintense sig-
nal involving the central cord from C1 downwards.
Journal of Medical Case Reports 2007, 1:4 http://www.jmedicalcasereports.com/content/1/1/4
Page 4 of 5
(page number not for citation purposes)
whereas in a relapse the cells should derive solely from the
girl. The donor-host chimerism of these CSF T-cells is of
note, since chimerism has been highlighted as a risk factor
for CNS relapse after allogeneic BMT for leukaemia.
Other CNS sequelae of acute leukaemia and its treatment
can also present with an acute encephalomyelopathy.
These include: medication toxicity (e.g. cyclosporin),
opportunistic CNS infection, secondary tumour, radiation
myelopathy, mineralising arteriopathy, necrotising leu-
koencephalopathy and graft-versus-host-disease (GVHD)
associated cerebral angiitis [1,4-6]. The majority of these
CNS sequelae have been reported within the first 12
months after treatment, although secondary tumours typ-
ically appear later. The initial MRI appearance in this girl
did not show the necrotizing or vacuolating appearance
found in the radiation-related sequelae. GVHD-associated
cerebral angiitis is an under-recognised entity which can
appear as a late syndrome after allogeneic BMT. It can
present with haemorrhagic or infarctive stroke, or a demy-
elinating encephalomyelitis with similar neuroimaging
and CSF findings to those in our girl [5]. Unlike the previ-
ously reported patients with GVHD-associated cerebral
angiitis, our girl did not have systemic features to suggest
chronic GVHD.
Severe encephalomyelitis can be caused by herpesviruses,
aspergillus and toxoplasmosis [6]. These infections are
early rather than late sequelae, occurring during the
period of immunosuppression. Myelitis due to these
agents is uncommon in immunocompetent patients. It is
not possible to distinguish infective encephalomyelitis
from ADEM on MR imaging alone so we continued aciclo-
vir treatment in our patient pending the results of virology
investigations.
The combination of MR imaging appearances and exclu-
sion of other diagnoses led to the diagnosis of ADEM [2].
The classical lesions of ADEM on MRI are multifocal
lesions in the brain white matter, cortical grey matter and
basal ganglia as in our girl. Around 20% of children with
ADEM have spinal involvement, although total spinal
cord length involvement as seen in our girl is atypical.
The immunophenotyping of the girl's prominent CSF
lymphocytosis suggests that her ADEM was a T-cell driven
disease process. This a novel finding, and is in keeping
with a previous report of increased myelin reactivity in
peripheral blood T-cells from children recovering from
ADEM [7]. We suggest immunophenotyping with flow
cytometry of CSF cells from patients with ADEM may
reveal further insights into the immunopathogenesis of
this condition.
There have been a few previous reports of children and
adults with ADEM following BMT for various leukaemias
and lymphomas [1,8,9]. All of these cases of ADEM
occurred as an early sequel of allogeneic BMT, in the
weeks or months of immunosuppression following the
transplant. ADEM occurring several years after BMT, dur-
ing prolonged remission, has not previously been
reported.
We do not think it likely that the girl's ADEM was related
to the combination of cranial and total body irradiation
she received prior to her BMT. This combination has been
associated with brain atrophy on neuroimaging and vas-
cular sequelae (necrotizing leukoencephalopathy and cav-
ernomatous angiodyslasias), but neurological sequelae
overall were not significantly more common than in
patients who did not receive cranial irradiation [1]. In
Table 1: Differential diagnosis of acute encephalomyelopathy after bone marrow transplantation for leukaemia
Metabolic, nutrient and electrolyte disturbances
Treatment side-effects
Cyclosporin (posterior leukoencephalopathy syndrome)
Amphotericin (parkinsonism)
Radiation sequelae (arteriopathy, vacuolating encephalomyelopathy)
Infections
Viruses (HSV, VZV, CMV, EBV, HHV6, HHV7, JC, BK, adenovirus, West Nile Virus)
Parasites (Toxoplasma, amoeba)
Fungi (Aspergillus, Candida)
Bacteria (abcesses, Listeria, Mycoplasma, TB)
CNS relapse of leukaemia
Inflammation
Acute disseminated encephalomyelitis
Multiple sclerosis
Vasculitides (SLE, CNS angiitis)
Haemorrhage/infarction
Thrombocytopoenic thrombotic purpura
Secondary to radiation arteriopathy
Idiopathic subarachnoid and subdural haemorrhage
Publish with BioMed Central and every
scientist can read your work free of charge
"BioMed Central will be the most significant development for
disseminating the results of biomedical research in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
Journal of Medical Case Reports 2007, 1:4 http://www.jmedicalcasereports.com/content/1/1/4
Page 5 of 5
(page number not for citation purposes)
addition ADEM and cerebral angiitis, both immunologi-
cal sequelae, following BMT have been reported in
patients who received only total body irradiation without
cranial irradiation [5,9].
Could this girl have been predisposed to developing
ADEM by her bone marrow transplantation? This is a fea-
sible hypothesis. Autoimmune disorders may have an
increased incidence after allogeneic BMT [10]. Guillain-
Barré disease, a peripheral neurological disorder with an
autoimmune component, has been reported as an early
sequel in post-BMT patients [6]. As noted above, ADEM
also has an autoimmune component with peripheral T-
cells from children with ADEM show increased reactivity
to host myelin basic protein [7]. It is possible that the BMT
may induce a susceptibility to an environmental trigger
for ADEM. We suggest that children who have received all-
ogeneic BMT should be monitored for immune-mediated
neurological disorders as part of long-term follow-up.
Conclusion
Acute disseminated encephalomyelitis should be consid-
ered as an alternative to leukaemic relapse in patients with
an acute encephalomyelopathy after allogeneic bone mar-
row transplantation. Demyelinating syndromes such as
acute disseminated encephalomyelitis may be a late
sequelae of bone marrow transplantation.
Competing interests
The author(s) declare that they have no competing inter-
ests.
Authors' contributions
RK and SN summarised the patient notes. RK and JG
reviewed the existing literature. RK wrote the manuscript
with review by JG and OI. All authors were involved in the
clinical care of the patient. All authors read and approved
the final manuscript.
Acknowledgements
Written consent was obtained from the patient for publication of the
report.
References
1. Faraci M, Lanino E, Dini G, Fondelli MP, Morreale G, Dallorso S, Man-
zitti C, Calevo MG, Gaggero R, Castagnola E, Haupt R: Severe neu-
rologic complications after hematopoietic stem cell
transplantation in children. Neurology 2002, 59(12):1895-1904.
2. Tardieu M, Mikaeloff Y: What is acute disseminated encephalo-
myelitis (ADEM)? Eur J Paediatr Neurol 2004, 8(5):239-242.
3. Au WY, Lie AK, Liang R, Kwong YL: Isolated extramedullary
relapse of acute lymphoblastic leukaemia after allogeneic
bone marrow transplantation. Bone marrow transplantation 1999,
24(10):1137-1140.
4. Chen CY, Zimmerman RA, Faro S, Bilaniuk LT, Chou TY, Molloy PT:
Childhood leukemia: central nervous system abnormalities
during and after treatment. Ajnr 1996, 17(2):295-310.
5. Ma M, Barnes G, Pulliam J, Jezek D, Baumann RJ, Berger JR: CNS
angiitis in graft vs host disease. Neurology 2002,
59(12):1994-1997.
6. Denier C, Bourhis JH, Lacroix C, Koscielny S, Bosq J, Sigal R, Said G,
Adams D: Spectrum and prognosis of neurologic complica-
tions after hematopoietic transplantation. Neurology 2006,
67(11):1990-1997.
7. Pohl-Koppe A, Burchett SK, Thiele EA, Hafler DA: Myelin basic
protein reactive Th2 T cells are found in acute disseminated
encephalomyelitis. Journal of neuroimmunology 1998, 91(1-
2):19-27.
8. Woodard P, Helton K, McDaniel H, Khan RB, Thompson S, Hale G,
Benaim E, Kasow K, Leung W, Horwitz E, Srivastava DK, Tong X,
Yusuf U, Cunningham JM, Handgretinger R: Encephalopathy in
pediatric patients after allogeneic hematopoietic stem cell
transplantation is associated with a poor prognosis. Bone mar-
row transplantation 2004, 33(11):1151-1157.
9. Tomonari A, Tojo A, Adachi D, Iseki T, Ooi J, Shirafuji N, Tani K,
Asano S: Acute disseminated encephalomyelitis (ADEM)
after allogeneic bone marrow transplantation for acute mye-
loid leukemia. Annals of hematology 2003, 82(1):37-40.
10. Sherer Y, Shoenfeld Y: Autoimmune diseases and autoimmu-
nity post-bone marrow transplantation. Bone marrow transplan-
tation 1998, 22(9):873-881.


![Báo cáo seminar chuyên ngành Công nghệ hóa học và thực phẩm [Mới nhất]](https://cdn.tailieu.vn/images/document/thumbnail/2025/20250711/hienkelvinzoi@gmail.com/135x160/47051752458701.jpg)























%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)