BioMed Central
Page 1 of 4
(page number not for citation purposes)
Journal of Medical Case Reports
Open Access
Case report
Synchronous colonic carcinomas presenting as an inguinoscrotal
hernial mass: a case report
Siao Pei Tan*, Siong-Seng Liau, Shayma'u M Habeeb and Dermot O'Riordan
Address: Department of General Surgery, West Suffolk Hospital, Hardwick Lane, Bury St Edmunds, IP33 2QZ Suffolk, UK
Email: Siao Pei Tan* - siaopei@gmail.com; Siong-Seng Liau - liauss@doctors.org.uk; Shayma'u M Habeeb - shaymau2001@yahoo.com;
Dermot O'Riordan - Dermot.O'Riordan@wsh.nhs.uk
* Corresponding author
Abstract
Background: A carcinoma within a hernia in the groin is uncommon, with an incidence of less
than 0.5 percent of all excised sacs. This article describes a case of synchronous colonic carcinomas,
one of which presented as an inguinoscrotal mass.
Case presentation: A 69-year old man presented with a large, irreducible left inguinoscrotal
hernia and symptoms of obstruction. On examination, there was an 8 cm palpable mass within the
hernia sac. CT scan revealed small and proximal large bowel obstruction secondary to a large
ingunoscrotal sac and synchronous colonic tumours of the transverse colon and the ascending
colon. The former presented as an inguinoscrotal mass. Laparotomy revealed a large tumour mass
arising from the transverse colon in the hernia sac. The procedure was followed by an extended
right hemicolectomy, during which the second tumour in the ascending colon was also resected.
Conclusion: This case demonstrates a rare but interesting occurrence of primary transverse
colon carcinoma presenting in a hernia sac, in conjunction with a synchronous tumour of the
ascending colon. Prognosis is comparable to patients with a solitary tumour of similar pathological
staging when the resection is curative. The presence of an inguinal hernia itself does not signify an
increased risk of colorectal malignancy. However, in the presence of obstruction, incarceration,
and weight loss, malignancy should be suspected. Thorough clinical examination, flexible
sigmoidoscopy or radiographic evaluation is necessary preoperatively in such patients. Surgical
resection, with or without adjuvant oncological treatment, should be performed as soon as
possible, using established techniques with modifications according to involvement of local
structures.
Background
Carcinomas in hernias in the groin are divided into saccu-
lar, intrasaccular and extrasaccular [1], based on the ana-
tomical relation to the sac. A saccular tumour is when the
primary or metastatic disease directly involves the perito-
neal sac, (for example a mesothelioma or peritoneal
metastases from other organs). Intrasaccular tumour
occurs when the incarcerated hernia contains an organ
with a primary carcinoma. The commonest of these cases
is a sigmoid colon carcinoma presenting in the left
inguinal hernia [2]. Hernia contents of urological and
gynaecological origin are also possible. We report the first
case reported in the literature with one of two synchro-
nous primary tumours presenting within a hernia, and to
Published: 28 June 2007
Journal of Medical Case Reports 2007, 1:36 doi:10.1186/1752-1947-1-36
Received: 23 February 2007
Accepted: 28 June 2007
This article is available from: http://www.jmedicalcasereports.com/content/1/1/36
© 2007 Tan et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Medical Case Reports 2007, 1:36 http://www.jmedicalcasereports.com/content/1/1/36
Page 2 of 4
(page number not for citation purposes)
our best knowledge, the first description of a primary
tumour of the transverse colon presenting in an inguinal
hernia.
Case presentation
A 69-year old man with a long-standing irreducible left
inguinoscrotal hernia presented with 6–8 weeks history of
constant dull ache in the paraumbilical region and associ-
ated vomiting. He also reported having loose stools and
weight loss of 2 stone over the last 6–8 weeks. On exami-
nation, there was a large irreducible left inguinoscrotal
hernia with a palpable mass measuring approximately 8
cm within the hernia sac. Plain abdominal film revealed
evidence of subacute small bowel obstruction. A subse-
quent CT revealed small and proximal large bowel
obstruction with a large left-sided inguinoscrotal hernia.
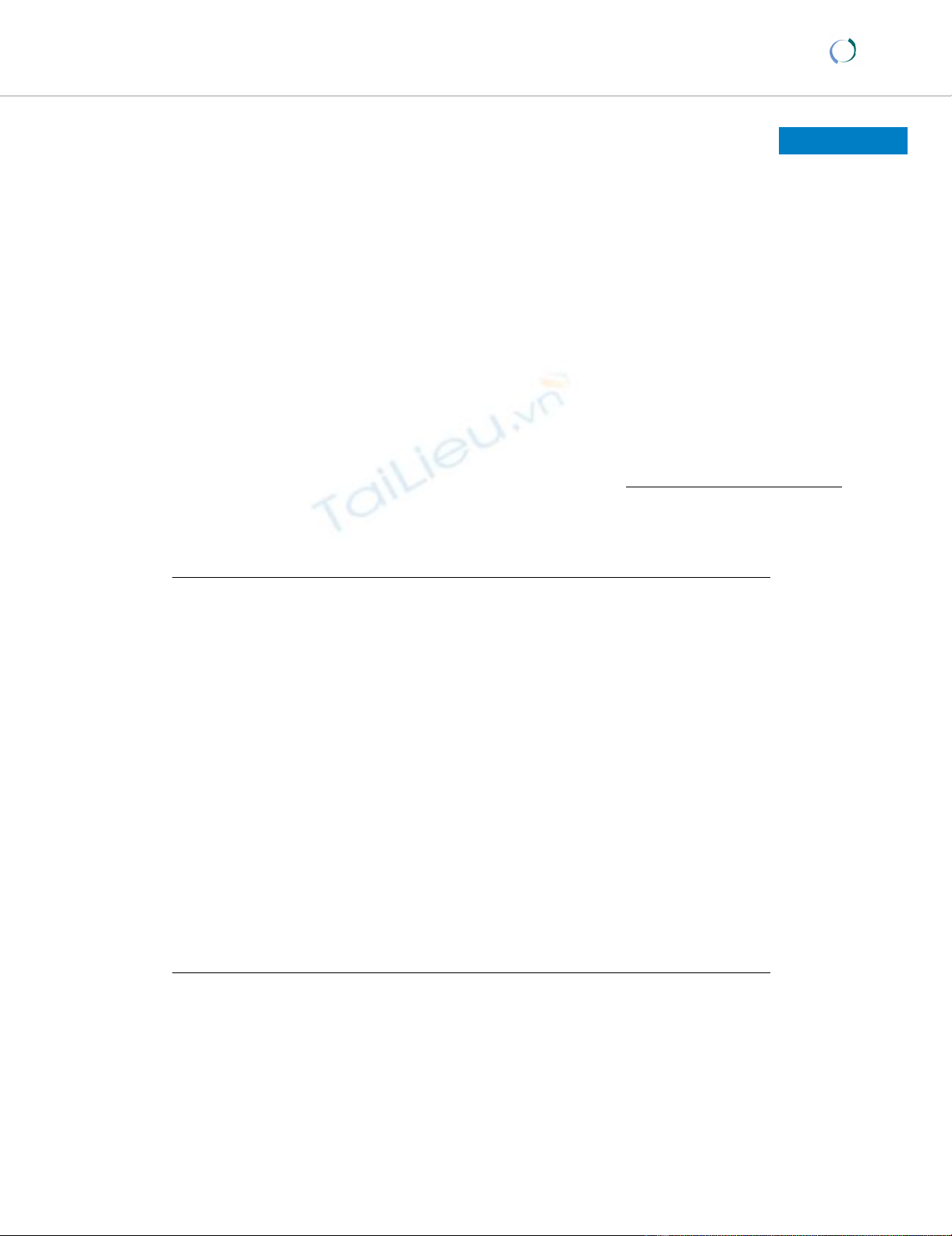
In addition, there was a loop of transverse colon, with sig-
nificant circumferential wall thickening, within the hernia
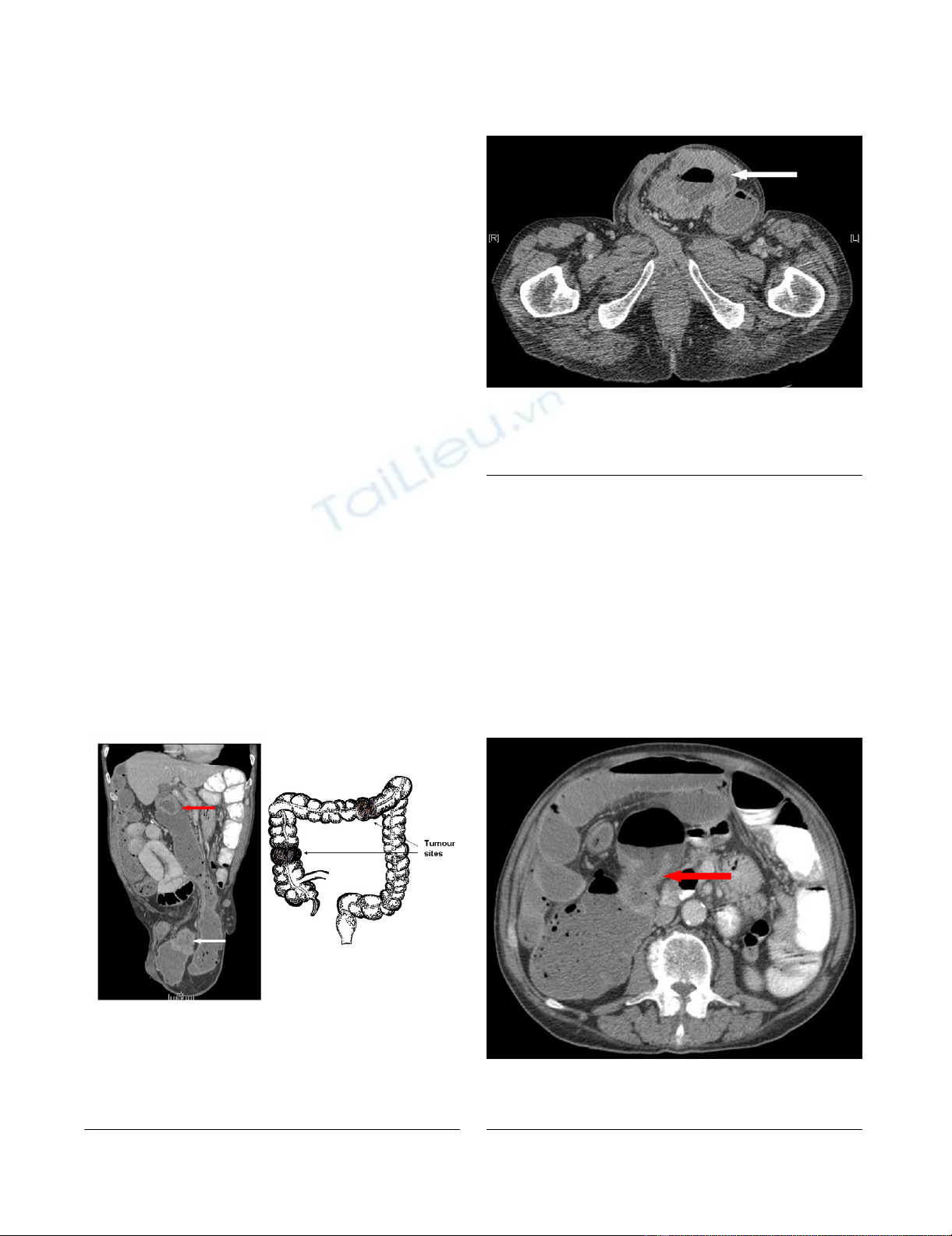
sac (See Figure 1 and 2). There was also a second area of
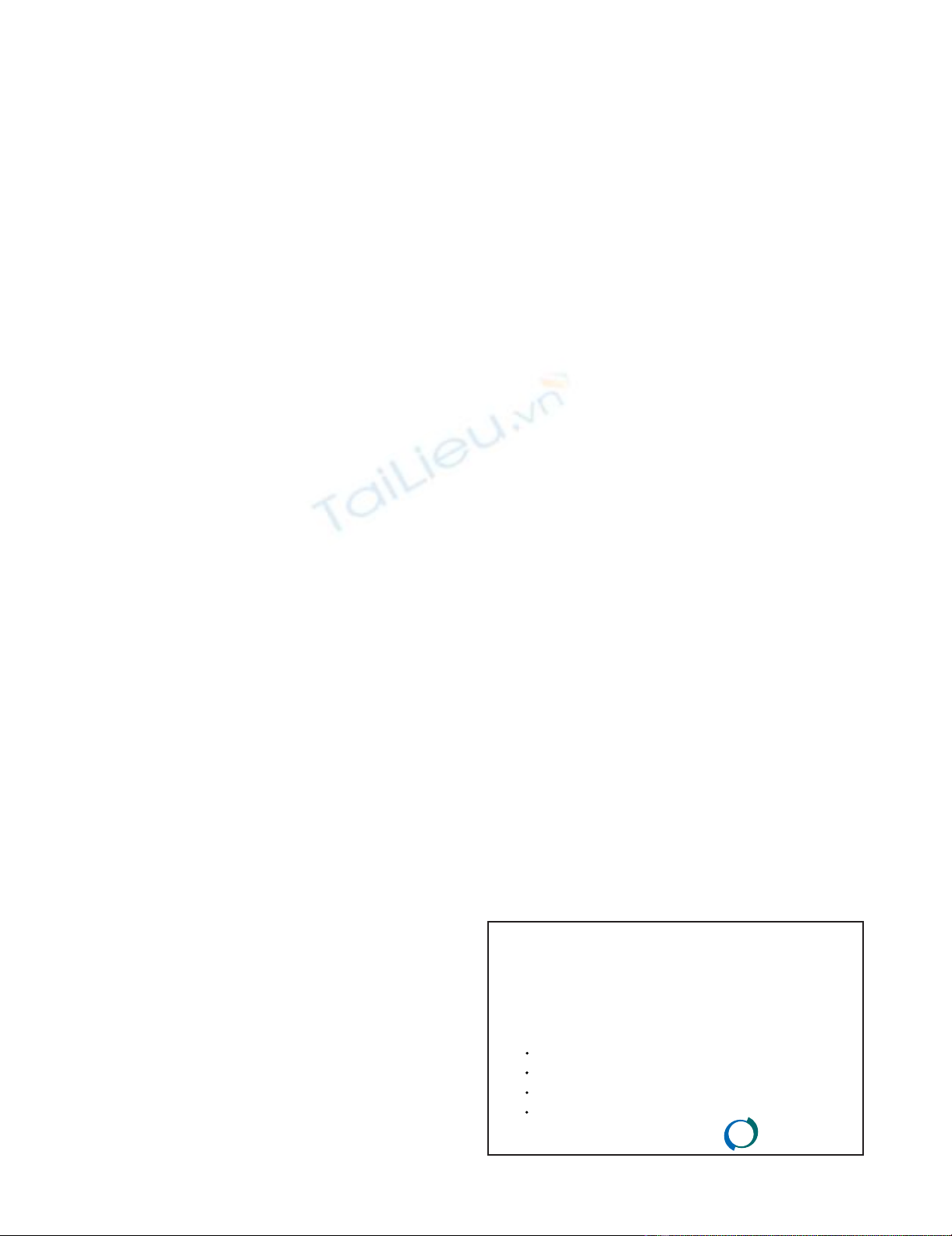
circumferential bowel wall thickening with narrowing
seen in the region of the hepatic flexure (See Figure 1 and
3). There were no signs of liver metastases or abdominal
lymphadenopathy. A full pre-operative metastatic survey
and assessment of the entire colon was not performed as
he was acutely unwell with bowel obstruction. At laparot-
omy, it was evident that there were synchronous tumours
in the transverse colon close to the splenic flexure and at
the ascending colon. The former presented as a mass in an
incarcerated left inguinoscrotal hernia. The hernial sac
was reduced following release of the external oblique with
a groin incision.
Surgical techniques
Under general and epidural anaesthesia, the patient was
placed in the supine position. A midline laparotomy was
performed and revealed grossly distended small and large
bowel. After an attempt at reducing the incarcerated left
inguinoscrotal hernia failed, an incision was made at the
left groin to release the external oblique and the hernia
was reduced without breach of the hernial sac. The groin
incision allowed visualisation of the cord structures and
there were no gross signs of tumour invasion locally. A
large tumour mass arising from the transverse colon was
found in the hernia sac. A further tumour was found at the
Imaging of the abdomen (cross sectional)Figure 3
Imaging of the abdomen (cross sectional). CT scan
showing tumour of the ascending colon (red arrow).
Imaging of the abdomen (coronal view)Figure 1
Imaging of the abdomen (coronal view). Left: CT scan
showing tumours of the ascending colon, seen at the hepatic
flexure (red arrow), and of the transverse colon (white
arrow), seen in the left inguinoscrotal hernia sac. Right: Dia-
grammatic representation of the tumour sites.
Imaging of the abdomen (cross sectional)Figure 2
Imaging of the abdomen (cross sectional). CT scan
showing tumour of the transverse colon (white arrow) pre-
senting within a left inguinoscrotal hernia.

Journal of Medical Case Reports 2007, 1:36 http://www.jmedicalcasereports.com/content/1/1/36
Page 3 of 4
(page number not for citation purposes)
ascending colon. The procedure was followed by an
extended right hemicolectomy with primary ileo-colonic
anastomosis. Good margins from both tumours were
allowed. A 10-cm section of terminal ileum was excised.
Small bowel with interloop adhesion was dissected and
freed. The terminal ileum was anastomosed to the
descending colon with TLC 75 staples to form a side-to-
side functional end-to-end anastomosis.
Histological examination confirmed a moderately differ-
entiated adenocarcinoma (pT3 N0 Mx; Dukes B) of the
ascending colon with one focus of extramural vascular
invasion. The second tumour was again a moderately dif-
ferentiated adenocarcinoma of the transverse colon with
one focus of extramural vascular invasion (pT3 N0 Mx;
Dukes B). All 14 lymph nodes showed no evidence of
nodal metastases.
Convalescence was initially complicated by reduced urine
output which was managed with fluid balance and use of
furosemide. He made a slow but good recovery and was
discharged on day 37. The case was discussed in a multi-
disciplinary meeting. In view of the vascular invasion, a
post-discharge oncology outpatient appointment was
arranged to discuss the option of adjuvant chemotherapy.
He will also be offered left sided colon imaging, either
colonoscopy or flexible sigmoidoscopy, to assess the
remainder of the colon.
Discussion
The incidence of synchronous malignancies of the colon
and rectum varies from 2 to 11 percent. We need to detect
synchronous malignancies, if any, during resection of the
index lesions in order to avoid repeated surgery in the
future, at which time the tumours are more likely to be of
advanced stage and thus bear a less favourable prognosis.
We can do this by performing preoperative total colonos-
copy, palpating the entire colon intraoperatively, and
carefully inspecting the resected segment macroscopically
and microscopically after the operation [3].
Most synchronous tumours arise as independent neo-
plasms. They are generally similar to single lesions in clin-
ical characteristics and pathological findings [3].
However, one study has shown that the male:female ratio
was higher and distant metastasis was more frequent in
synchronous than in single cases [3]. In a study involving
876 patients where 42 cases (4.8%) were synchronous car-
cinomas, postoperative survival was significantly shorter
in synchronous cases than in single cases on univariate
analysis. Nonetheless, in the multivariate proportional
hazard model in which pathological stage and curability
were included as prognostic co-factors, the difference in
postoperative survival between the two groups was insig-
nificant [3]. As such, the prognosis of those with synchro-
nous tumours is similar to those with solitary colon
tumours on a stage-for-stage basis when the resections are
curative [3] and the highest stage synchronous tumour is
considered [4].
There is limited literature on the management of patients
with malignancies in hernia sacs and we found no clear
evidence on the best approach in treating these patients.
The previously reported cases were mainly of sigmoid
tumours [5] and to our best knowledge, this is the first
reported case of a primary tumour of the transverse colon
presenting in an inguinal hernia, in addition to a synchro-
nous tumour at the ascending colon. Intraoperatively, the
colonic attachments at the splenic flexure were intact. We
speculate that mechanical factors probably played a sig-
nificant role in the process of herniation of the tumour. It
is possible that the tumour served as a point of propulsion
and was aided by gravity to herniate at the inguinal
region.
Invasion of the contiguous structures within a hernial sac
in not unheard of [6]. Lymphatic spread to preaortic
nodes via gonadal vessels has been reported, especially
when the spermatic cord is involved [6]. This situation
warrants a more radical resection and adjuvant oncologi-
cal treatment. In this present case, through the groin inci-
sion, there was no gross evidence to suggest cord
involvement. However, in view of the microscopic vascu-
lar invasion, the patient was offered a post-discharge
oncology outpatient appointment to discuss the option of
adjuvant chemotherapy.
The reported increased incidence of colonic malignancies
in inguinal hernia patients that exceeds the age-related
expected incidence has led some to advocate screening
[7]. Gravity [2], raised intra-abdominal pressure second-
ary to the tumour development, straining on defaecation
or partial intestinal obstruction have been said to contrib-
ute to the development of hernias. However, studies have
found no causative relationship between inguinal hernia
and colonic malignancies [8,9]. The current consensus is
that patients with inguinal hernias should undergo
screening for colon cancer at the same rate as the general
population [10]. Nonetheless, a previously reducible her-
nia with associated symptoms such as obstruction, anae-
mia, weight loss, or change in bowel habit, should raise a
high index of suspicion for colonic malignancies. Investi-
gation such as barium enema, colonoscopy or a CT scan
would be appropriate in these situations.
Conclusion
The present case demonstrates a rare but interesting occur-
rence of primary transverse colon carcinoma presenting in
a hernia sac, in conjunction with a synchronous tumour
of the ascending colon. The presence of an inguinal hernia
Publish with BioMed Central and every
scientist can read your work free of charge
"BioMed Central will be the most significant development for
disseminating the results of biomedical research in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
Journal of Medical Case Reports 2007, 1:36 http://www.jmedicalcasereports.com/content/1/1/36
Page 4 of 4
(page number not for citation purposes)
itself does not signify an increased risk of colorectal malig-
nancy. Further, inguinal hernia alone is a relatively rare
cause of colonic obstruction. In the present case, the pres-
ence of symptoms of obstruction, incarceration, weight
loss and a palpable mass within the hernia sac immedi-
ately raised the suspicion of malignancy. Thorough clini-
cal examination, endoscopic (e.g colonoscopy) and
radiological evaluations (e.g abdominal CT scan) are nec-
essary preoperatively in such patients. Surgical resection,
with or without adjuvant oncological treatment, should
be performed as soon as possible, using established tech-
niques with modifications according to involvement of
local structures. Prognosis is comparable to patients with
a solitary tumour of similar pathological staging when the
resection is curative.
Competing interests
The author(s) declare that they have no competing inter-
ests.
Authors' contributions
SPT drafted the article, prepared the illustration and per-
formed the literature search. SSL assisted in performing
the surgery, conceived this report, and supervised drafting
and revision of the article. SMH helped to acquire the
radiological images, prepared the cover letter and per-
formed the literature search. DOR performed the surgery,
supervised the drafting and overall structure of the article.
All authors have read and approved the final manuscript.
Acknowledgements
We would like to thank Dr Eivind Carlsen (pathology) and Dr Laura
Watson (radiology) for their help and support.
Authors are not funded by any source in the writing and submission of the
article.
Written consent was obtained from the patient for presentation and pub-
lication of the study, including the radiological images.
References
1. Lejars J: Neoplasmes herniaires et peri-herniaires. Gaz Hosp
1889, 62:801-811.
2. Matsumoto G, Ise H, Inoue H, Ogawa H, Suzuki N, Matsuno S: Met-
astatic colon carcinoma found within an inhuinal hernia sac:
Report of a case. Surg Today 2000, 30:74-77.
3. Oya M, Takahashi S, Okuyama T, Yamaguchi M, Ueda Y: Synchro-
nous colorectal carcinoma: Clinico-pathological features and
prognosis. Japanese Journal of Clinical Oncology 2003, 33:38-43.
4. Passman MA, Pommier RF, Vetto JT: Synchronous colon prima-
ries have the same prognosis as solitary colon cancers. Dis-
eases of the colon and rectum 1996, 39(3):329-334.
5. Boormans JL, Hesp WLEM, Teune TM, Plaisier PW: Carcinoma of
the sigmoid presenting as a right inguinal hernia. Hernia 2006,
10:93-96.
6. Tan GY, Guy RJ, Eu KW: Obstructing sigmoid cancer with local
invasion in an incarcerated inguinal hernia. ANZ J Surg 2003,
73:80-82.
7. Lovett J, Kirgan D, McGregor B: Inguinal hernia justifies sig-
moidoscopy. Am J Surg 1989, 158:615-617.
8. Brendel TH, Kirsh IE: Lack of association between inguinal her-
nia and carcinoma of the colon. N Eng J Med 1971,
284(7):369-370.
9. Juler GL, Stemmer EA, Fullerman RW: Inguinal hernia and color-
ectal carcinoma. Arch Surgery 1972, 104(6):778-780.
10. Gerson LB, Triadafilopoulos G: Is colorectal cancer screening
necessary in the preoperative assessment of inguinal herni-
orrhaphy? A case-control study. The American Journal of Gastro-
enterology 2001, 96(6):1914-1917.



![PET/CT trong ung thư phổi: Báo cáo [Năm]](https://cdn.tailieu.vn/images/document/thumbnail/2024/20240705/sanhobien01/135x160/8121720150427.jpg)






















%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)