BioMed Central
Page 1 of 6
(page number not for citation purposes)
World Journal of Surgical Oncology
Open Access
Case report
Hepatobiliary cystadenoma exhibiting morphologic changes from
simple hepatic cyst shown by 11-year follow up imagings
Naoto Fukunaga*1, Masashi Ishikawa1, Hisashi Ishikura1,
Toshihiro Ichimori1, Suguru Kimura1, Akihiro Sakata1, Koichi Sato2,
Jyunichi Nagata2 and Yoshiyuki Fujii3
Address: 1Department of Surgery, Tokushima Red Cross Hospital, Komatsushima-City, Tokushima Prefecture, Japan, 2Department of
Gastroenteology, Tokushima Red Cross Hospital, Komatsushima-City, Tokushima Prefecture, Japan and 3Department of Pathology, Tokushima
Red Cross Hospital, Komatsushima-City, Tokushima Prefecture, Japan
Email: Naoto Fukunaga* - naotowakimachi@hotmail.co.jp; Masashi Ishikawa - masa1192@tokushima-med.jrc.or.jp;
Hisashi Ishikura - masa1192@tokushima-med.jrc.or.jp; Toshihiro Ichimori - masa1192@tokushima-med.jrc.or.jp;
Suguru Kimura - masa1192@tokushima-med.jrc.or.jp; Akihiro Sakata - masa1192@tokushima-med.jrc.or.jp; Koichi
Sato - masa1192@tokushima-med.jrc.or.jp; Jyunichi Nagata - masa1192@tokushima-med.jrc.or.jp; Yoshiyuki Fujii - masa1192@tokushima-
med.jrc.or.jp
* Corresponding author
Abstract
Background: A long-term follow up case of hepatobiliary cystadenoma originating from simple
hepatic cyst is rare.
Case presentation: We report a case of progressive morphologic changes from simple hepatic
cyst to hepatobiliary cystadenoma by 11 – year follow up imaging. A 25-year-old man visited our
hospital in 1993 for a simple hepatic cyst. The cyst was located in the left lobe of the liver, was 6
cm in diameter, and did not exhibit calcification, septa or papillary projections. No surgical
treatment was performed, although the cyst was observed to gradually enlarge upon subsequent
examination. The patient was admitted to our hospital in 2004 due to epigastralgia. Re-examination
of the simple hepatic cyst revealed mounting calcification and septa. Abdominal CT on admission
revealed a hepatic cyst over 10 cm in diameter and a high-density area within the thickened wall.
MRI revealed a mass of low intensity and partly high intensity on a T1-weighted image. Abdominal
angiography revealed hypovascular tumor. The serum levels of AST and ALT were elevated slightly,
but tumor markers were within normal ranges. Left lobectomy of the liver was performed with
diagnosis of hepatobiliary cystadenoma or hepatobiliary cystadenocarcinoma. The resected
specimen had a solid component with papillary projections and the cyst was filled with liquid-like
muddy bile. Histologically, the inner layer of the cyst was lined with columnar epithelium showing
mild grade dysplasia. On the basis of these findings, hepatobiliary cystadenoma was diagnosed.
Conclusion: We believe this case provides evidence of a simple hepatic cyst gradually changing
into hepatobiliary cystadenoma.
Published: 11 December 2008
World Journal of Surgical Oncology 2008, 6:129 doi:10.1186/1477-7819-6-129
Received: 28 July 2008
Accepted: 11 December 2008
This article is available from: http://www.wjso.com/content/6/1/129
© 2008 Fukunaga et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
World Journal of Surgical Oncology 2008, 6:129 http://www.wjso.com/content/6/1/129
Page 2 of 6
(page number not for citation purposes)
Background
Hepatobiliary cystadenoma is a rare benign tumor arising
from the liver, or less frequently from the extrahepatic bil-
iary tree. Edmondson et al [1]. reported the definition of
the hepatobiliary cystadenoma for the first time in 1958.
It accounts for 4.6% of intrahepatic cysts of bile duct ori-
gin and the most frequently occurs in middle-aged
women[2]. In 1985, Wheeler and Edmondson[3]
described distinct criteria for hepatobiliary cystadenoma
based on the presence or absence of mesenchymal stroma.
Cystadenoma lacking mesenchymal stroma predomi-
nantly occurred in males while cystadenoma with mesen-
chymal stroma is composed of intermediate stroma
components and is most prevalent in females. It is charac-
terized by multilocular cyst with a solid component,
septa, papillary projections, or mural nodules[4].
Although the clinical and pathological findings of hepato-
biliary cystadenoma and cystadenocarcinoma have been
well-described, it cannot be distinguished from one
another by imaging findings including computed tomog-
raphy (CT), magnetic resonance imagings (MRI) and
ultrasound (US). Moreover, hepatobiliary cystadenoma
and simple hepatic cysts can change into hepatobiliary
cystadenocarcinoma with time[2,5]. Although his-
topathological differentiation between hepatobiliary cys-
tadenoma and cystadenocarcinoma is indisputable, it is
unknown whether hepatobiliary cystadenocarcinomas
arise de-novo come or whether they arise from hepatobil-
iary cystadenomas. A long-term follow up study of hepa-
tobiliary cystadenoma may contribute to the clarification
of this sequence. Herein, we report a case of hepatobiliary
cystadenoma with morphologic changes from simple
hepatic cyst by 11-year follow up imaging.
Case presentation
A simple hepatic cyst was detected in the left lobe of the
liver of a 25-year-old man in 1993 (Sadly, there was no
imaging.). The patient was followed in our hospital, and
no surgical treatment was performed although the cyst
showed gradual enlargement. The patient was admitted to
our hospital due to epigastralgia and for re-examination
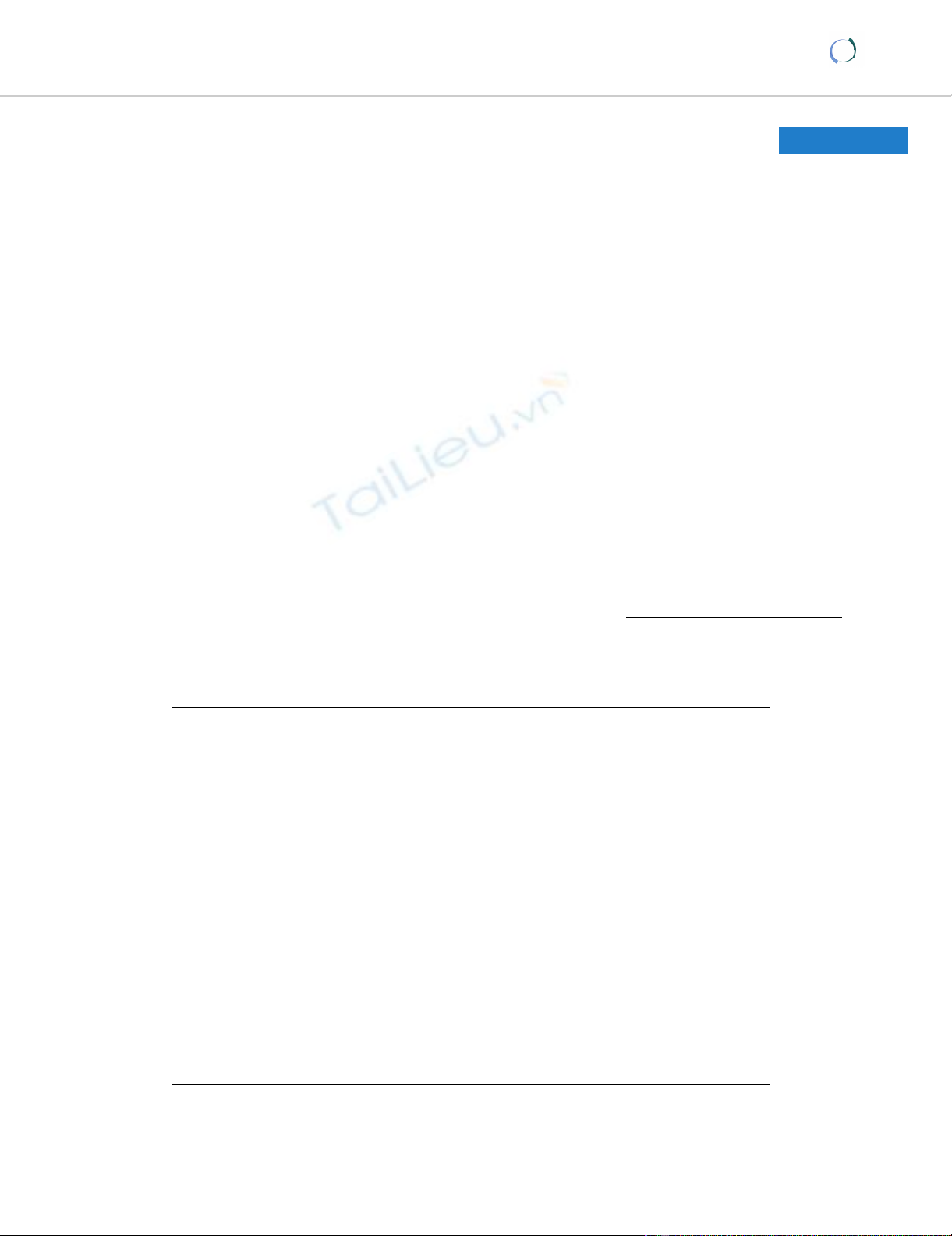
of simple hepatic cyst in 2004. In 1996 the cyst was
unilocular, 6 cm in diameter without calcification, septa
or papillary projections as observed by CT (Fig. 1a). In
2001 the cyst remained the same diameter but exhibited
calcification and septa (Fig. 1b). An abdominal CT per-
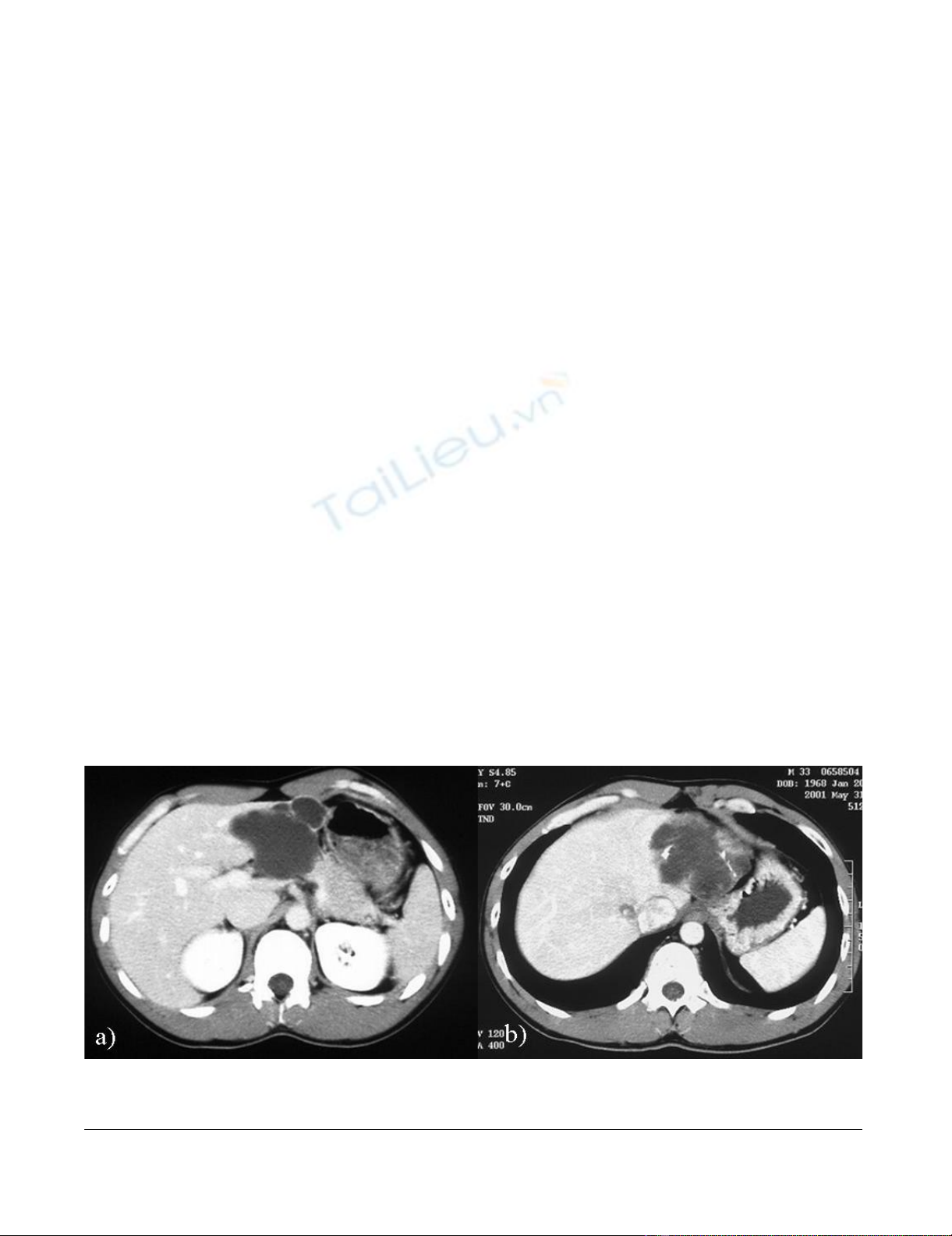
formed on admission in 2004 showed that the unilocular
cyst had grown to over 10 cm in diameter with increasing
mounting calcification, septa and thickening of the wall
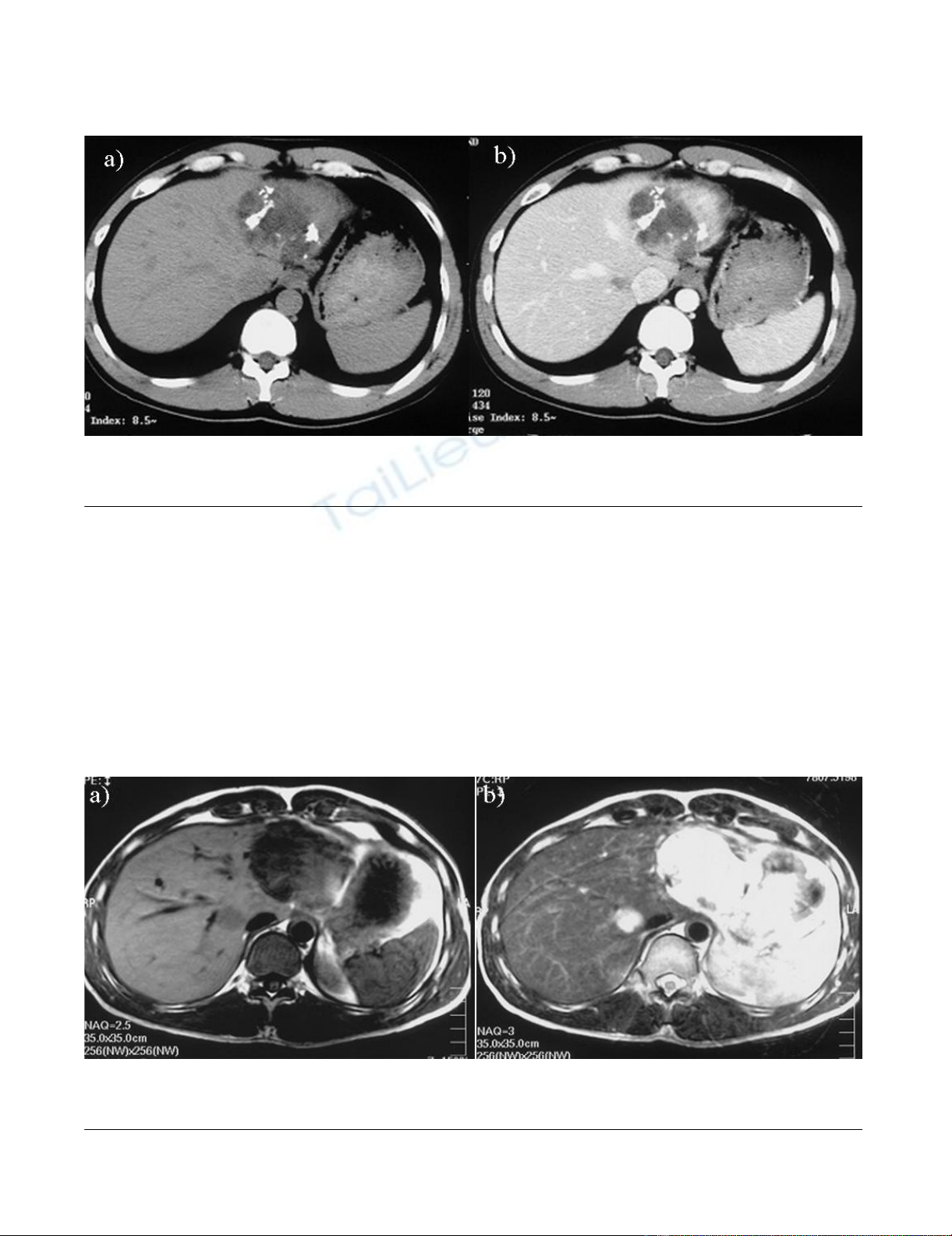
within the cyst (Fig. 2a, b). MRI revealed a partly low
intensity, partly high intensity T1-weighted image, and
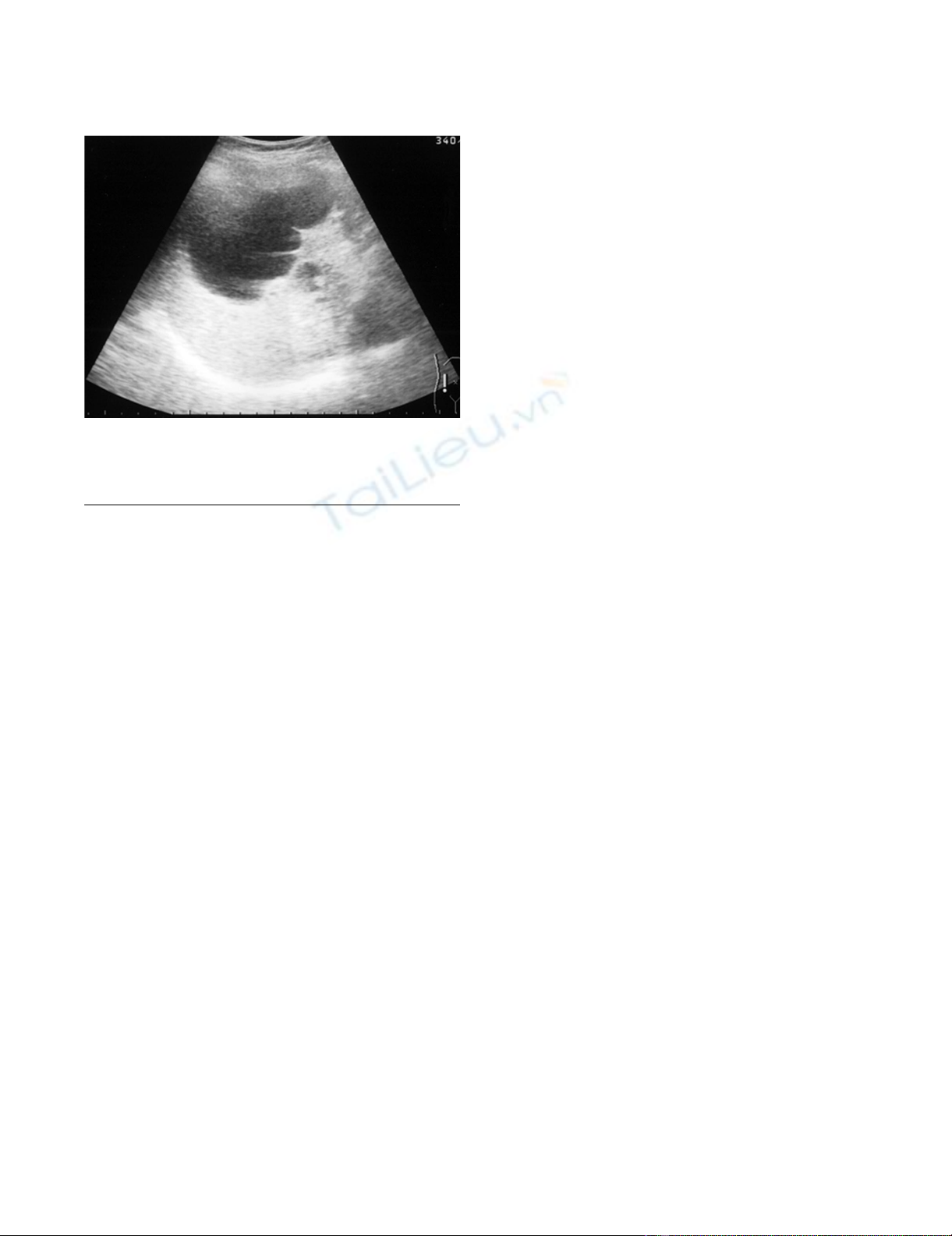
high intensity T2-weighted image (Fig. 3a, b). US revealed
a unilocular cyst over 10 cm in diameter and partial septa
within the cyst (Fig. 4). Abdominal angiography showed
the tumor to be hypovascular and stretching of left hepatic
artery. Endoscopic retrograde cholangiopancreatography
(ERCP) revealed compression of the bile duct and no
communication between the cyst and the bile duct was
shown. The serum level of aspartame aminotransferase
(AST) and almandine aminotransferase (ALT) were
slightly elevated but tumor markers such as CEA and CA
19-9 were within the normal range. The cystic lesion was
suspected of being a mucin-producing liver tumor, such as
hepatobiliary cystadenoma or cystadenocarcinoma.
Despite of these findings, we could not rule out the malig-
nancy clearly. Therefore, in November 2004, left lobec-
tomy of the liver with cholecystectomy was performed.
Abdominal CT findingsFigure 1
Abdominal CT findings. a) in 1996, showing the unilocular cyst 6 cm in diameter without calcification, septa and papillary
projections. No contrast enhancement was seen. b) in 2001, showing the same diameter with calcification and septa.
World Journal of Surgical Oncology 2008, 6:129 http://www.wjso.com/content/6/1/129
Page 3 of 6
(page number not for citation purposes)
Macroscopically, a resected specimen was a unilocular
tumor filled with mucus. The cut surface of the tumor
exhibited an elastic white-colored scar and yellowish pap-
illary nodule (Fig. 5a). The unilocular cyst had a solid
component with papillary projections, septa and calcifica-
tion and was filled with liquid-like muddy bile. His-
topathological examination revealed that the inner layer
of the cyst was lined columnar epithelium exhibiting mild
grade dysplasia and partially lined with papillary epithe-
lium (Fig. 5b). Dense mesenchymal stroma was not
detected. On the basis of these findings, hepatobiliary cys-
tadenoma was diagnosed. The postoperative course was
uneventful and recurrence of the lesion has not been
observed. We believe this case provides evidence of a sim-
ple hepatic cyst changing into hepatobiliary cystadenoma
over a 10-year period.
Discussion
Hepatobiliary cystadenoma is a rare benign tumor arising
from the epithelium [2]. Hepatobiliary cystadenoma is
reported to be defined as multilocular cystic tumors lined
with columnar epithelium and containing dense cellular
stroma.
Abdominal CT findings in 2004Figure 2
Abdominal CT findings in 2004. a) showing the unilocular cyst over 10 cm in diameter, increasing eruplioid calcification,
septa and thickness of the wall within the cyst. b) the contrast was seen a little at the left side of the cyst.
Abdominal MRI in 2004, showing the unilocular cyst 10 cm in diameterFigure 3
Abdominal MRI in 2004, showing the unilocular cyst 10 cm in diameter. a) low intensity, partly high intensity on T1-
weighted image, b) high intensity on T2-weighted image were seen.
World Journal of Surgical Oncology 2008, 6:129 http://www.wjso.com/content/6/1/129
Page 4 of 6
(page number not for citation purposes)
In general, hepatobiliary cystadenoma was described as
multilobular cyst with smooth surfaces and the vascula-
ture externally [3]. The tumor tissue was also described
such as white, grey – white, pink and so on. The internal
surface of the tumor was generally smooth with occa-
sional trabeculations, sessile or polypoid cysts. Hepatobil-
iary cystadenoma containted clear or turbid fluid
described as mucinous or gelatinous, which was quanti-
fied from 700 to 4200 ml.
As to microscopic features in details, hepatobiliary cystad-
enoma consisted of following three layers; 1) the epithe-
lial layer of mucin producing columnar to cuboidal cells
lining within the cysts; 2) the layer, less than 3 mm in
thickness of undifferentiated mesenchmal cells; 3) the
outer layer, which was the dense layer with collagenous
connective tissue.
Tumor size varies from 8 to 20 cm, with a mean of 13 cm
[6]. Symptoms are various, including an upper abdominal
mass, epigastralgia and abdominal pain. Asymptomatic
lesions may be discovered incidentally during radiologi-
cal or surgical procedures for unrelated conditions. Jaun-
dice due to compression of the bile duct [6] and ascites
due to compression of the vena cava and hepatic vein are
rare. Laboratory examination is normal in most patients,
although some exhibit mild elevated serum liver enzymes
due to compression of the cystic mass. Tumor markers are
also not unusually elevated, although Lee et al [7],
revealed high serum CA 19-9 and the presence of CA 19-9
and CEA in the epithelial component of hepatobiliary cys-
tadenoma by immunohistochemical analysis. Our case
exhibited frequent symptoms and was diagnosed with a
simple hepatic cyst by US and CT in 1993, although the
cystic mass showed enlargement with internal septa and
papillary projections. The characteristic CT findings of
hepatobiliary cystadenoma are low-density well-sub-
scribed masses with internal septa, mural nodules and
papillary projections [4,6]. Contrast enhancement is often
seen along the internal septa and wall. The US findings are
also ovoid, cystic masses with multiple echogenic septa
and papillary projections along the wall or septa [4,6,8].
Takayasu et al [8], have reported that US and CT are useful
tools to clarify internal structure of the tumors and that
make it easy to determine the preoperative diagnosis, but
Matsumoto et al [4], reported that with regard to the inter-
nal structure, US was superior to CT in demonstration of
internal morphology. Our case showed enlargement of
the cyst with internal septa and papillary projections and
emerging dense calcification along the wall and internal
septa, being atypical of hepatobiliary cystadenoma. In
particular, the presence of calcification along the wall or
septa was reported to indicate hepatobiliary cystadenocar-
cinoma[4]. MRI is useful to evaluate the contents of the
cysts such as mucin or hemorrhage[4]. ERCP is often used
to show communication between hepatobiliary cystade-
noma and intrahepatic duct. In some cases, a communica-
tion between the biliary tract and the tumor are shown by
ERCP or intraoperative cholangiography. Angiographic
findings are not diagnostic, but stretching of the hepatic
arteries and irregular calibers of the peripheral arteries in
the arterial phase and stains in the parenchymal phase
lead to the suspicion of malignancy[9]. Hepatobiliary cys-
tadenoma should be suspected by neovascularity with a
thin rim of contrast material accumulating within the
cysts[8]. Furthermore, in general, hemorrhagic internal
fluid is suggestive of hepatobiliary cystadenocarcinoma,
whereas mixed or mucinous fluid is suggestive of hepato-
biliary cystadenoma. Certainly, imaging findings charac-
teristic of hepatobiliary cystadenoma are recognized, but
the differential diagnosis between hepatobiliary cystade-
noma and hepatobiliary cystadenocarcinoma on the basis
of imaging findings alone has not been established [4].
Some hepatobiliary cystadenoma and simple hepatic cysts
are reported to show malignant transformation into hepa-
tobiliary cystadenocarcinoma after a number of
years[2,5]. As mentioned above, hepatobiliary cystade-
noma was classified based on the presence or absence of
mesenchymal stroma. Cystadenoma with mesenchymal
stroma, which occured in females had the malignant
transformation into cystadenocarcinoma with stromal
invasion. There has been the possible histogenesis, respec-
tively. Devaney et al[10], divided hepatobiliary cystaden-
ocarcinoma into two groups; 1) that arising from
preexisting cystadenoma with mesenchymal stroma,
which predominantly occurred in females with an indo-
lent clinical course; 2) that not associated with preexisting
cystadenoma mesenchymal stroma, which occurred in
Abdominal US in 2004, showing the unilocular cyst over 10 cm in diameterFigure 4
Abdominal US in 2004, showing the unilocular cyst
over 10 cm in diameter. Partially, the septa within the
cyst were seen.

World Journal of Surgical Oncology 2008, 6:129 http://www.wjso.com/content/6/1/129
Page 5 of 6
(page number not for citation purposes)
males having an extremely aggressive clinical course. On
the other hand, hepatobiliary cystadenoma with mesen-
chymal stroma may arise from ectopic ovary incorporated
into the liver or ectopic rests of primitive tissue such as
embryonic gallbladder and bile ducts, while that without
mesenchymal stroma may originate from bile buct epithe-
lium as reactions induced by various stimuli[3]. Ishak et
al[2], reported the theories of origin of hepatic cyst. We
speculated our case without mesenchymal stroma was
originated from simple hepatic cyst as reactions by some
stimuli, which were not unknown. Akiyoshi et al[11],
reported a case of hepatobiliary cystadenocarcinoma with
progression from a benign cystic lesion over 12 years. In
their case, a small cyst grew by only 3 cm in diameter over
12 years and become malignant. We considered that
malignant formation was not related to the rate of
increase in the size of the cyst and took the malignancy
based on the presence of calcification, malignant poten-
tial of benign cysts reported and the recurrence of hepato-
biliary cystadenoma despite the presence of mesenchymal
stroma into consideration. In our case, the progressive
morphologic changes including enlargement of the cyst
from 6 cm to 10 cm, septa, increasing calcification and
thickness of the wall was recognized. Therefore, we per-
formed the complete surgical resection. Kosuge et al[12],
reported that the postoperative recurrence in patients who
underwent radical resection for hepatobiliary cystadeno-
carcinoma was much less than that of patients with other
hepatic malignancies. In our case, the surgical margin was
negative and long-term survival would be expected. The
benefit of chemotherapy has not still established in
patients with palliative resection or distant metastasis.
Conclusion
We report a case of hepatobiliary cystadenoma with mor-
phologic changes from simple hepatic cyst shown by 11-
year follow up imagings. Fortunately, complete radical
resection was performed and no recurrence has been
observed to date. Complete resection is mandatory surgi-
cal procedure, when hepatobiliary cystadenoma showing
atypical imaging findings is suspected, or the malignancy
cannot be denied.
Consent
Written informed consent was obtained from the for pub-
lication of this case report and any accompany images. A
copy of written consent is available for review by the Edi-
tor-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
NF wrote this manuscript and revised it. MI performed the
operation. He conceptualize and recommended me to
write this case and advised me to revise it. HI performed
the operation and conceptualize and recommended me to
write this case. TI performed the operation and conceptu-
alize and recommended me to write this case. SK per-
formed the operation and conceptualize and
recommended me to write this case. AS performed the
operation and conceptualize and recommended me to
write this case. KS participated in the design of this case.
JN participated in the design. YF made a diagnosis of this
case histologically and participated in the design. All
authors read and approved the final manuscript.
Cut surface and pathological findings in 2004Figure 5
Cut surface and pathological findings in 2004. a) Cut surface, showing elastic white-colored scar and yellowish papillary
nodule. b) Pathological finding, showing the inner layer of the cyst was lined with a columnar epithelium exhibiting mild grade
dysplasia, partially with a papillary epithelium.


























%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)