BioMed Central
Page 1 of 4
(page number not for citation purposes)
World Journal of Surgical Oncology
Open Access
Technical innovations
Management of malignant pleural effusion and ascites by a triple
access multi perforated large diameter catheter port system
Ihsan Inan*1, Sandra De Sousa†1, Patrick O Myers†1, Brigitte Bouclier†2,
Pierre-Yves Dietrich†2, Monica E Hagen†1 and Philippe Morel†1
Address: 1Visceral Surgery Division, Department of Surgery, Geneva University Hospital, Rue Micheli-du-Crest 24, CH-1211, Geneva, Switzerland
and 2Oncology Department, Geneva University Hospital, Rue Micheli-du-Crest 24, CH-1211, Geneva, Switzerland
Email: Ihsan Inan* - ihsan.inan@hcuge.ch; Sandra De Sousa - sandra.desousa@hcuge.ch; Patrick O Myers - patrick.myers@hcuge.ch;
Brigitte Bouclier - brigitte.bouclier@hcuge.ch; Pierre-Yves Dietrich - pierre-yves.dietrich@hcuge.ch; Monica E Hagen - monika.hagen@hcuge.ch;
Philippe Morel - philippe.more@hcuge.ch
* Corresponding author †Equal contributors
Abstract
Background: Pleural or peritoneal effusions (ascites) are frequent in terminal stage malignancies.
Medical management may be hazardous.
Methods: A 60-year-old man with metastatic malignant melanoma presented refractory ascites as
well as bilateral pleural effusions. After failure of the medical treatment, bilateral pleural aspiration
and paracentesis became necessary two to three times a week. A multi perforated 15F silicone
catheter connected with a subcutaneous port was implanted in peritoneal and both pleural cavities
surgically under general anesthesia. Leakage around the catheter is prevented by subcutaneous
tunneling. Surgical technique is described and illustrated in a video.
Results: Implanted systems were immediately operational. Follow up period was 41 days. Each
port was accessed 10 times and a total of 65'200 ml of fluid was drained. By the end of the forth
week, pleural effusions diminished, systems were controlled for permeability and chest x-rays
confirmed absence of effusion.
Conclusion: Implanted port systems for refractory ascites and pleural effusions avoid morbidity
and the patient's anxiety related to repeated puncture-aspiration. Large catheter diameter allows
an easy and fast drainage of large volumes. Compared to chronic indwelling catheters,
subcutaneous location of port system allows an entire integration, giving the patient a total liberty
in daily life between two sessions of drainage. Drainage can be performed in an outpatient basis as
an ambulatory procedure. This patient-friendly technique may be a treatment option in case of
failure of other techniques.
Background
Pleural effusion and ascites are frequent in terminal stage
malignancies. In the United States, patients affected by
malignant pleural effusions alone is estimated to 175'000
per year [1]. Fluid sequestration significantly compro-
mises patient's quality of life.
Published: 18 August 2008
World Journal of Surgical Oncology 2008, 6:85 doi:10.1186/1477-7819-6-85
Received: 24 February 2008
Accepted: 18 August 2008
This article is available from: http://www.wjso.com/content/6/1/85
© 2008 Inan et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

World Journal of Surgical Oncology 2008, 6:85 http://www.wjso.com/content/6/1/85
Page 2 of 4
(page number not for citation purposes)
Almost 75% of all malignant pleural effusions are due to
malignancies of breasts, lungs, ovaries and lymphomas.
Malignant pleural effusions account for approximately
40% of chronic pleuritis cases. They are mostly recurrent
and often resistant to systemic treatment. They occur
mainly from obstruction or disruption of lymphatic chan-
nels by malignant cells.
In case of symptomatic malignant pleural effusion, dysp-
nea (moderate to severe, according to the importance of
the effusion), cough, thoracic discomfort as well as pain
may be present [2].
Malignant ascites leads to shortness of breath, nausea,
diminished appetite and early satiety, fatigue, lower
extremity edema, limited mobility and difficulty to fit
clothes. Ascites results from multiple mechanisms includ-
ing vascular permeability changes, peritoneal carcinoma-
tosis (metastatic implants of carcinoma on the peritoneal
cavity), lymph drainage obstruction, hepatic congestion
due to tumour infiltration or neoplastic production of
exudative fluid [3]. Ascites may develop in various circum-
stances but mainly in cirrhosis and peritoneal carcinoma-
tosis. Complication may arise, such as respiratory
restriction and respiratory distress under diaphragmatic
compression (elevation of diaphragm, compressing the
lung and reducing their compliance), spontaneous bacte-
rial peritonitis, electrolyte and hemodynamic distur-
bances, hepatorenal syndrome, physical discomfort with
limitation of the movements leading to reduction of the
quality of life [4,5].
The aim of treatment is to improve the quality of life by
decreasing these symptoms. We report our experience
with a patient presenting both pleural and peritoneal effu-
sions. Multiperforated large diameter, totally implanted
port systems were surgically inserted in each cavity. The
clinical course of the patient is summarized, treatment
options discussed and surgical technique is described in a
video file.
Clinical experience
A 60-year-old man known for a malignant melanoma
since 1999 developed a small bowel metastasis in 2003.
Since he was detected as HIV, stage III A+ in 2002, he was
not integrated in specific immunotherapy programs and
no other treatment was proposed. In 2005, he presented
with refractory ascites as well as bilateral pleural effusions.
Patient refused any kind of pleurodesis. A central venous
access port was implanted and he received three cycles of
chemotherapy (Vinblastine, Dacarbazine and Cisplatine).
This measure also failed and the patient required perito-
neal paracentesis and thoracentesis 2 to 3 times a week. In
2006, the patient was referred by his oncologist and the
decision was made to insert multiperforated large diame-
ter, totally implanted port systems into the peritoneal and
both pleural cavities. Chronic indwelling pleural or peri-
toneal catheter systems available (PleurX™) were dis-
cussed and not retained neither by the patient nor by
oncologist because of inability of the patient to learn to
manage systems at the end stage of malignancy. Access
system implantationPatient informed about the tech-
nique before scheduling the operation. Procedure was
realized under standard balanced general anaesthesia
(Additional files 1, 2, and 3).
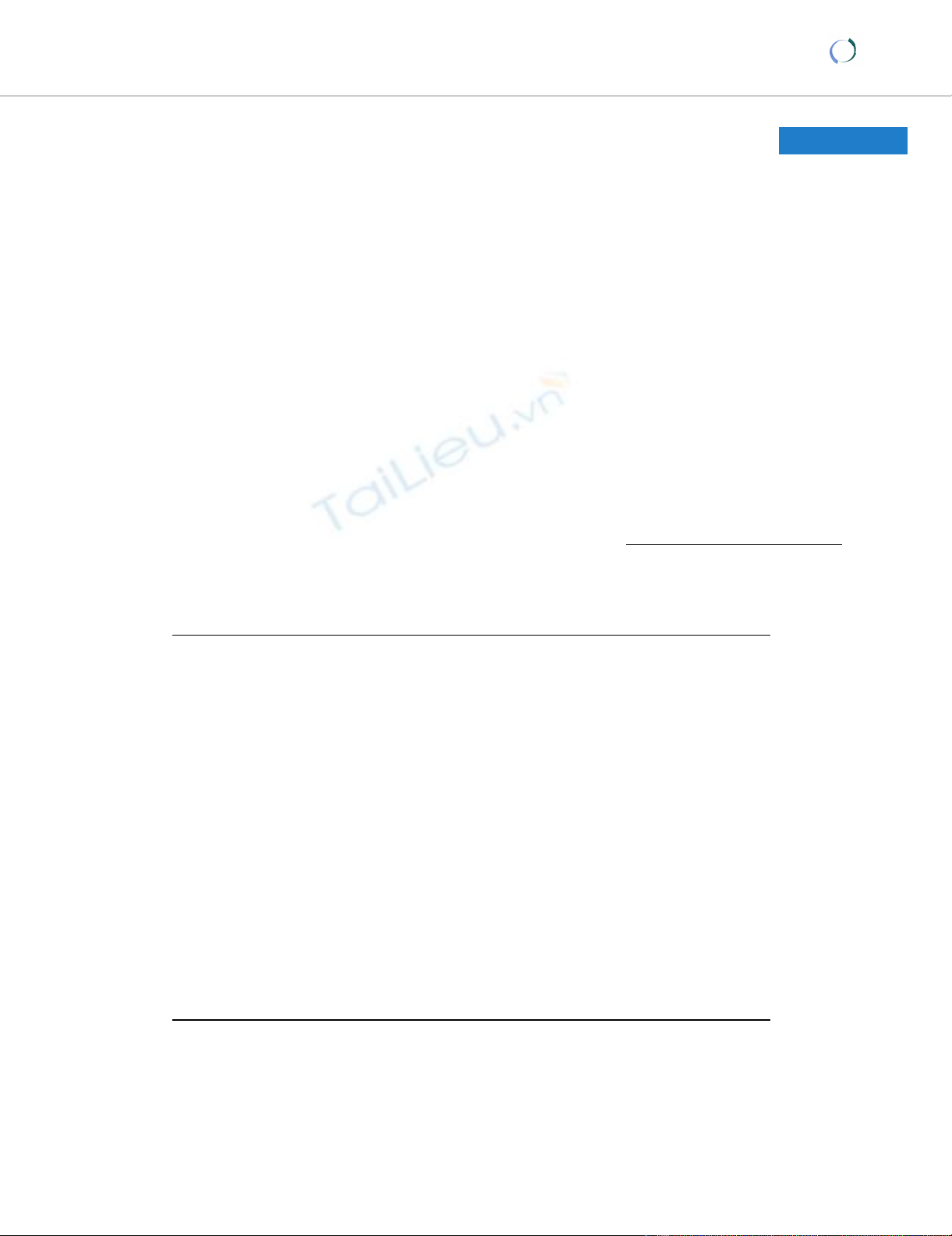
A Celsite T203J (B. Braun Medical SA, Sempach, Switzer-
land) port system with multi perforated large diameter sil-
icone catheter (outer diameter: 4.9 mm, inner diameter:
2.6 mm) with two Dacron cuffs (Figure 1) was first
implanted into the peritoneal cavity by a muscle splitting
transrectal incision. The catheter was positioned in the
right paracolic space. Patient received 20 g. of albumin per
two litres of peritoneal and pleural effusion. Volume
replacement and hemodynamic status monitored by
anesthesia team stayed stable during whole procedure. A
purse string suture was placed on the peritoneum and tied
around the Dacron cuff to insure watertight sealing, in
order to prevent leakage. A second incision was made on
the right costal margin at the anterior axillary line and a 3-
cm subcutaneous pocket created on the thoracic wall. The
catheter was passed to the proximal incision with a tun-
nelling device and connected to the port. The reservoir
was anchored on the anterior thoracic fascia by monofila-
ment non-absorbable 2.0 sutures. Identical systems were
placed in each pleural cavity with the same open surgical
technique. A chest x-ray at the end of the procedure in the
recovery room showed correct position of the catheters
and no residual pneumothorax. The follow up period was
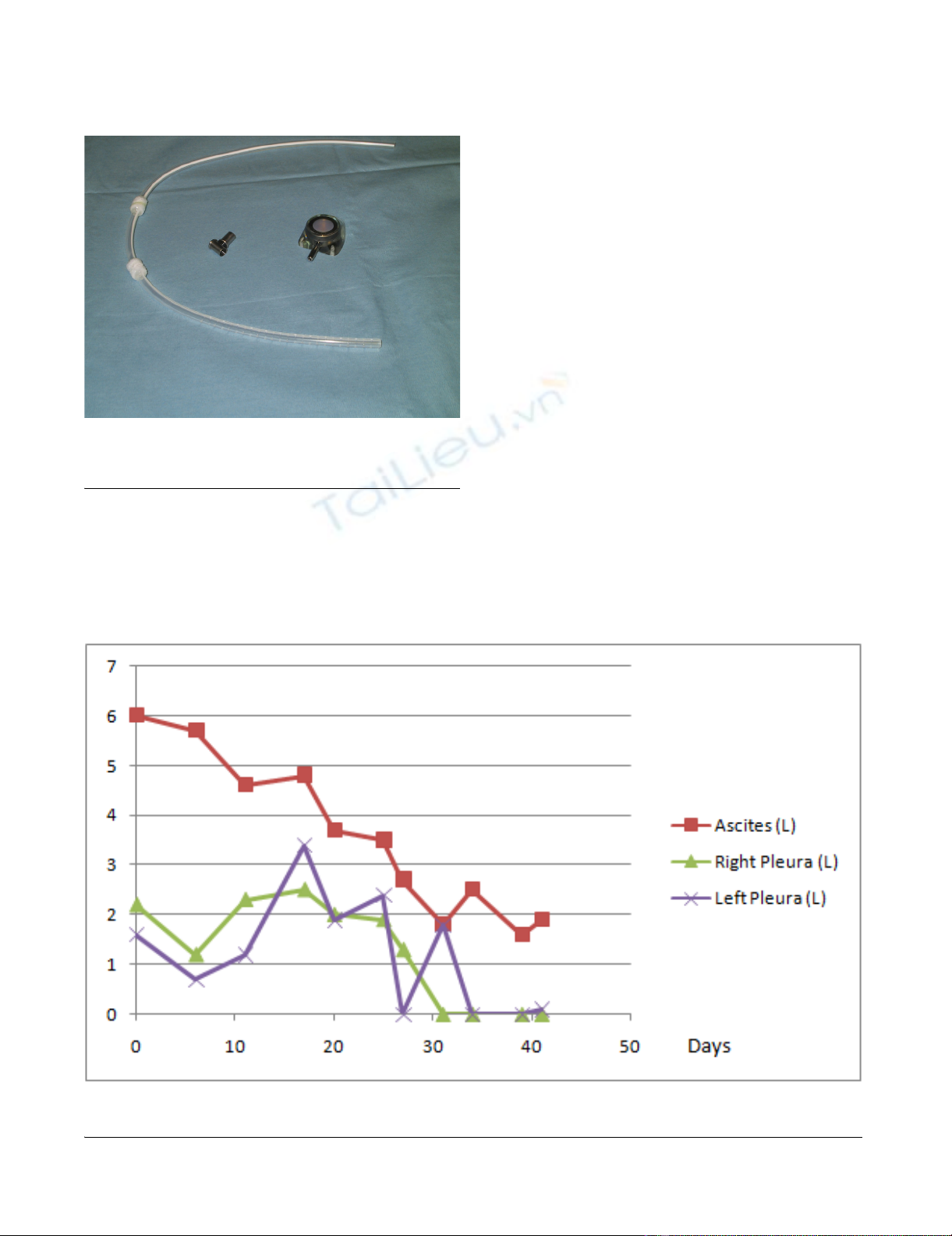
41 days. Each port was accessed 10 times and 65'200 ml
of fluid was drained. Effusion drainage was carried out by
using a peritoneal dialysis recipient system placed distally
and connected to a 1.1 × 19 mm Huber needle. It lasted
2h30 on average for volumes ranging from 600 ml to
5'700 ml (Figure 2). By the end of the forth week, pleural
effusions diminished, systems were controlled for perme-
ability and chest x-rays confirmed absence of effusions.
All care was given as a day procedure, without hospital
stay; the patient continued his daily activities normally
and maintained a good quality of life until his last days.
Death occurred due to brain metastasis, 7 weeks after the
implantation of the triple access system.
Discussion
There are several attitudes to manage pleural and abdom-
inal intracavitary refractory effusions in end stage patients
[6]. The aim of the treatment is to improve quality of life
by decreasing symptoms. First line treatment is therapeu-
tic pleural aspiration. In case of relapse or delayed man-
agement, repetitive pleural aspiration may be necessary.
World Journal of Surgical Oncology 2008, 6:85 http://www.wjso.com/content/6/1/85
Page 3 of 4
(page number not for citation purposes)
Repeated pleural aspiration may be complicated by pneu-
mothorax, bleeding, infection and spleen or liver lacera-
tion [7]. Pleurodesis, by mini thoracotomy or
thoracoscopy is favoured in patients with limited survival
[8]. Talc powder is preferred to other pleurodesis agents
like bleomycine, tetracycline or doxyciline, a tetracycline
analogue. Although unusual, effusion recurrence is possi-
ble early after pleurodesis, aspecially in high volume pleu-
ral effusions. When initial pleurodesis fails, there are
several alternatives to consider: repeated pleurodesis,
repeated pleural aspiration, systemic chemotherapy when
tumours are likely to respond to such a treatment, pleu-
roperitoneal shunting or pleurectomy. Surgical proce-
dures include parietal pleurectomy, or decortications.
Unfortunately, for different reasons, some patients may
not profit timely or do not benefit of pleurodesis. These
patients suffer both from compressive effect of effusions
between drainage sessions and from the risks and various
complications of repeated pleural punctures. In case of
failure or impossibility of pleurodesis, chronic indwelling
intercostal catheter implantation is described as an alter-
native. An implantable port system with multi perforated
large diameter catheter in the pleural cavity may be a treat-
ment alternative for end stage patients [9,10].
Ninety percent of patients with ascites respond to stand-
ard medical therapies, such as diuretics, sodium and water
restriction and diet. When ascites becomes chronic and
refractive to medical treatment, various possibilities are
available, such as aggressive diuretic therapy, high-vol-
ume paracentesis, ascites recirculation with peritoneov-
enous or intrahepatic portosystemic shunts [11].
Morbidity related to repeated abdominal puncture and
Multi perforated large diameter silicone catheter port system with two Dacron cuffsFigure 1
Multi perforated large diameter silicone catheter
port system with two Dacron cuffs.
Evolution of ascites and pleural fluid volume drainedFigure 2
Evolution of ascites and pleural fluid volume drained.
World Journal of Surgical Oncology 2008, 6:85 http://www.wjso.com/content/6/1/85
Page 4 of 4
(page number not for citation purposes)
paracentesis is well described, such as unsuccessful punc-
ture, pain, infection or even septicaemia and haemor-
rhage [12]. Frequent large volume paracentesis require
multiple visits to the healthcare facilities during the few
remaining months of life [13]. A peritoneovenous LeVeen
shunt may be complicated by pulmonary edema, presents
poor permeability at long term and may be complicated
by peritoneal fibrosis. Use of multi perforated large diam-
eter catheter with implantable port systems for refractory
ascites has several advantages. Large diameter of the cath-
eter allows an easy and fast drainage of large volumes.
Compared to chronic indwelling catheter systems, subcu-
taneous location of port system allows an entire corporeal
integration, giving the patient a total liberty in daily life
between two drainage sessions. Dacron cuffs placed on
the catheter insures hermetic sealing of the host cavity and
forms a barrier against infections.
Conclusion
In conclusion, in this particular case, managing malignant
pleural and peritoneal effusions with implanted large
diameter multiperforated port systems was successful.
This patient-friendly technique may be a treatment option
in case of failure of other treatment options.
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
II and SDS carried out the surgical care of the patient and
the follow-up during the treatment, realised the illustra-
tion and drafted the manuscript. POM, SDS, PYD, MH
participated to manuscript draft and literature research.
BB, PYD participated in the follow-up of the patient as
well as manuscript draft on oncologic aspect. MEH partic-
ipated to manuscript draft and literature research. PM
encouraged the case report, participated in its preparation
and helped to draft the manuscript. All authors read and
approved the final manuscript.
Additional material
Acknowledgements
None
References
1. Bennett R, Maskell N: Management of malignant pleural effu-
sions. Curr Opin Pulm Med 2005, 11:296-300.
2. Lee A, Lau TN, Yeong KY: Indwelling catheters for the manage-
ment of malignant ascites. Support Care Cancer 2000, 8:493-499.
3. Brooks RA, Herzog TJ: Long-term semi-permanent catheter
use for the palliation of malignant ascites. Gynecol Oncol 2006,
101:360-362.
4. Rosenblum DI, Geisinger MA, Newman JS, Boden TM, Markowitz D,
Powell D, Mullen KD: Use of subcutaneous venous access ports
to treat refractory ascites. J Vasc Interv Radiol 2001,
12:1343-1346.
5. Sabatelli FW, Glassman ML, Kerns SR, Hawkins IF Jr.: Permanent
indwelling peritoneal access device for the management of
malignant ascites. Cardiovasc Intervent Radiol 1994, 17:292-294.
6. Driesen P, Boutin C, Viallat JR, Astoul PH, Vialette JP, Pasquier J:
Implantable access system for prolonged intrapleural immu-
notherapy. Eur Respir J 1994, 7:1889-1892.
7. Antony VB, Loddenkemper R, Astoul P, Boutin C, Goldstraw P, Hott
J, Rodriguez PF, Sahn SA: Management of malignant pleural effu-
sions. Eur Respir J 2001, 18:402-419.
8. Antunes G, Neville E: Management of malignant pleural effu-
sions. Thorax 2000, 55:981-983.
9. Ohm C, Park D, Vogen M, Bendick P, Welsh R, Pursel S, Chmielewski
G: Use of an indwelling pleural catheter compared with tho-
rascopic talc pleurodesis in the management of malignant
pleural effusions. Am Surg 2003, 69:198-202.
10. Daniel C, Kriegel I, Di Maria S, Patrubani G, Levesque R, Livartowski
A, Esteve M: Use of a pleural implantable access system for
the management of malignant pleural effusion: the Institut
Curie experience. Ann Thorac Surg 2007, 84:1367-1370.
11. Ferral H, Bjarnason H, Wegryn SA, Rengel GJ, Nazarian GK, Rank JM,
Tadavarthy SM, Hunter DW, Castaneda-Zuniga WR: Refractory
ascites: early experience in treatment with transjugular int-
rahepatic portosystemic shunt. Radiology 1993, 189:795-801.
12. Verfaillie G, Herreweghe RV, Lamote J, Noppen M, Sacre R: Use of
a Port-a-Cath system in the home setting for the treatment
of symptomatic recurrent malignant pleural effusion. Eur J
Cancer Care (Engl ) 2005, 14:182-184.
13. Barnett TD, Rubins J: Placement of a permanent tunneled peri-
toneal drainage catheter for palliation of malignant ascites:
a simplified percutaneous approach. J Vasc Interv Radiol 2002,
13:379-383.
Additional file 1
Peritoneal and Pleural port compressed: Part 1
Click here for file
[http://www.biomedcentral.com/content/supplementary/1477-
7819-6-85-S1.mpg]
Additional file 2
Peritoneal and Pleural port compressed: Part 2
Click here for file
[http://www.biomedcentral.com/content/supplementary/1477-
7819-6-85-S2.mpg]
Additional file 3
Peritoneal and Pleural port compressed: Part 3
Click here for file
[http://www.biomedcentral.com/content/supplementary/1477-
7819-6-85-S3.mpg]


























%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)