Case report
Open Access
Well-differentiated gall bladder hepatoid carcinoma producing
alpha-fetoprotein: a case report
Ching-Yun Kao
1
*, Chian-Ro Chang
1
, Hung Chiang
2
, How-Tshung Chen
1
,
Shih-Ming Ma
1
and Che-Yu Cheng
1
Addresses:
1
West Garden Hospital, Taipei, Taiwan, ROC and
2
Taipei Institute of Pathology, Taipei, Taiwan, ROC
Email: CK* - cygau0308@yahoo.com.tw; CC - 0018@westgarden.com.tw; HC - joanne@mail.tipn.org.tw; HTC - 0026@westgarden.com.tw;
SM - docma@westgarden.com.tw; CYC - cycheng@westgarden.com.tw
* Corresponding author
Received: 17 August 2008 Accepted: 23 January 2009 Published: 26 June 2009
Journal of Medical Case Reports 2009, 3:7303 doi: 10.4076/1752-1947-3-7303
This article is available from: http://jmedicalcasereports.com/jmedicalcasereports/article/view/7303
© 2009 Kao et al; licensee Cases Network Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0),
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction: Gall bladder carcinoma is rare, and metastatic gall bladder carcinoma from
hepatocellular carcinoma has been reported in only a few patients.
Case presentation: We present a 73-year-old man with a history of hepatitis B virus-related liver
cirrhosis and hepatocellular carcinoma. He received transcatheter arterial chemoembolization, and
was diagnosed to have an alpha-fetoprotein producing gall bladder tumor with intraluminal growth.
Open cholecystectomy was performed. Pathologic examination of the lesion revealed a well-
differentiated hepatoid carcinoma. The lesion was thought most likely to be a metastatic lesion from
previous hepatocellular carcinoma. His alpha-fetoprotein level dropped to normal levels five months
after the surgery.
Conclusion: This unusual intraluminal growing tumor proved to be a well-differentiated hepatoid
carcinoma, most likely a metastatic lesion from previous hepatocellular carcinoma. This case reminds
clinicians that in looking for likely hepatocellular carcinoma recurrence, when no detectable hepatic
lesion can account for an elevated alpha-fetoprotein level, the gall bladder should be included in the
search for the site of metastasis.
Introduction
Gall bladder carcinoma is a rare disease, whether primary
or metastatic. It is usually diagnosed at a late stage due to
asymptomatic properties when small. Sometimes carci-
noma from the gall bladder also produces alpha-fetoprotein
(a-FP) because the gall bladder shares the same embryo-
logic origin as the liver. Only a handful of cases of a-FP
producing gall bladder carcinoma had been reported in the
literature, and many of them have been from Japan. Cell
types of these reported cases include clear cell carcinoma,
pleomorphic carcinoma or undifferentiated carcinoma.
Here we present a rare case of a well-differentiated gall
bladder hepatoid carcinoma producing a-FP after treatment
of primary hepatocellular carcinoma (HCC).
Page 1 of 4
(page number not for citation purposes)
Case presentation
A 73-year-old man visited our emergency room (ER) in
October 2004 with right upper abdominal pain and fever
for the previous two days. Vital signs on arrival at the ER
were blood pressure (BP): 161/107 mmHg, pulse rate
(PR): 90/minute, respiratory rate (RR): 20/minute, and
body temperature (BT): 38.9ºC. His consciousness was
unaffected but he had an acutely ill appearance. Tracing
back his medical history, he had hepatitis B virus (HBV)-
related liver cirrhosis (Child-Pugh Classification Grade A),
and in August 1999, a small HCC (Segment 5 of the liver,
diameter less than 2 cm) was diagnosed. He received
transcatheter arterial chemoembolization (TACE) at a
medical center and a second TACE again in May 2001
for recurrent HCC. He declined further TACE for residual
recurrent lesions. Therefore oral chemotherapy with the
regimen tegafur/uracil (100 mg/224 mg) had been
prescribed to him from December 2001 to November
2003, and was ceased due to loss at follow-up.
Physical examination in the ER found no yellowish skin, no
icteric sclera but moderate right upper quadrant (RUQ)
abdominal pain. Murphy’s sign was positive. Bowel sounds
were normal and his abdomen was soft, with no rebound-
ing pain. There was no shifting dullness. Lab data included:
white blood cell count (WBC): 14,520/mm
3
(Neu/Lym:
83.5/6.4%), platelets: 169 k/mm
3
, total and direct (T/D)
bilirubin: 1.4/0.6 mg/dL, serum glutamic-oxaloacetic trans-
aminase/serum glutamic-pyruvic transaminase (sGOT/
sGPT): 38/32 U/L, albumin (Alb): 3.9 gm/dL, C-reactive
protein: 11.9 mg/dL, NH
3
: 98 mcg/dL, and a-FP level:
231.1 ng/mL. Abdominal echogram revealed a thickened
gall bladder wall, gall stones and a suspected tumor mass
in the distended gall bladder. An abdominal computed
tomography (CT) scan showed liver cirrhosis, gall stones,
diffusely thickened gall bladder wall with increased contrast
enhancement compatible with acute cholecystitis, and a
hypodense mass lesion without contrast enhancement in
the gall bladder (Figure 1). There was no roentgenographic
evidence of a suspected recurrent lesion in the liver
parenchyma at that time.
An open cholecystectomy via a right subcostal incision
was performed on the next day. A distended gall bladder
with multiple pigmented gall stones and a tumor mass,
6.0 ¥4.0 ¥2.0 cm in size, were found in the gall bladder
lumen. When seen, the mass had already detached from
the mucosa at the opening of the sac and no stalk could be
identified (Figure 2, Panel A). The mucosal surface of the
gall bladder wall was smooth without evident tumorous
or ulcerative lesions (Figure 2, Panel B).
Microscopic pathologic examination of the gall bladder
revealed heavy neutrophil and lymphocyte infiltration as
in ordinary acute and chronic inflammation. The mucosa
was congested and showed no evidence of tumor invasion.
The vessels in the gall bladder wall were free from tumor
emboli (Figure 3, Panel A).
The sections of the tumor showed extensive infarction
necrosis. The viable tumor cells were seen as uniform
polygonal cells with eosinophilic granular cytoplasm
arranged in tiled array or microtrabecular pattern mostly
surrounding the blood vessels (Figure 3, Panel B and C).
Immunohistochemistry staining with a-FP antibody
demonstrated varied positive staining intensity in the
cytoplasm of the tumor cells (Figure 3, Panel D). Other
antibodies including CK7, chromogranin, and synapto-
physin were all negative, excluding the possibility of
carcinoid tumor or adenocarcinoma.
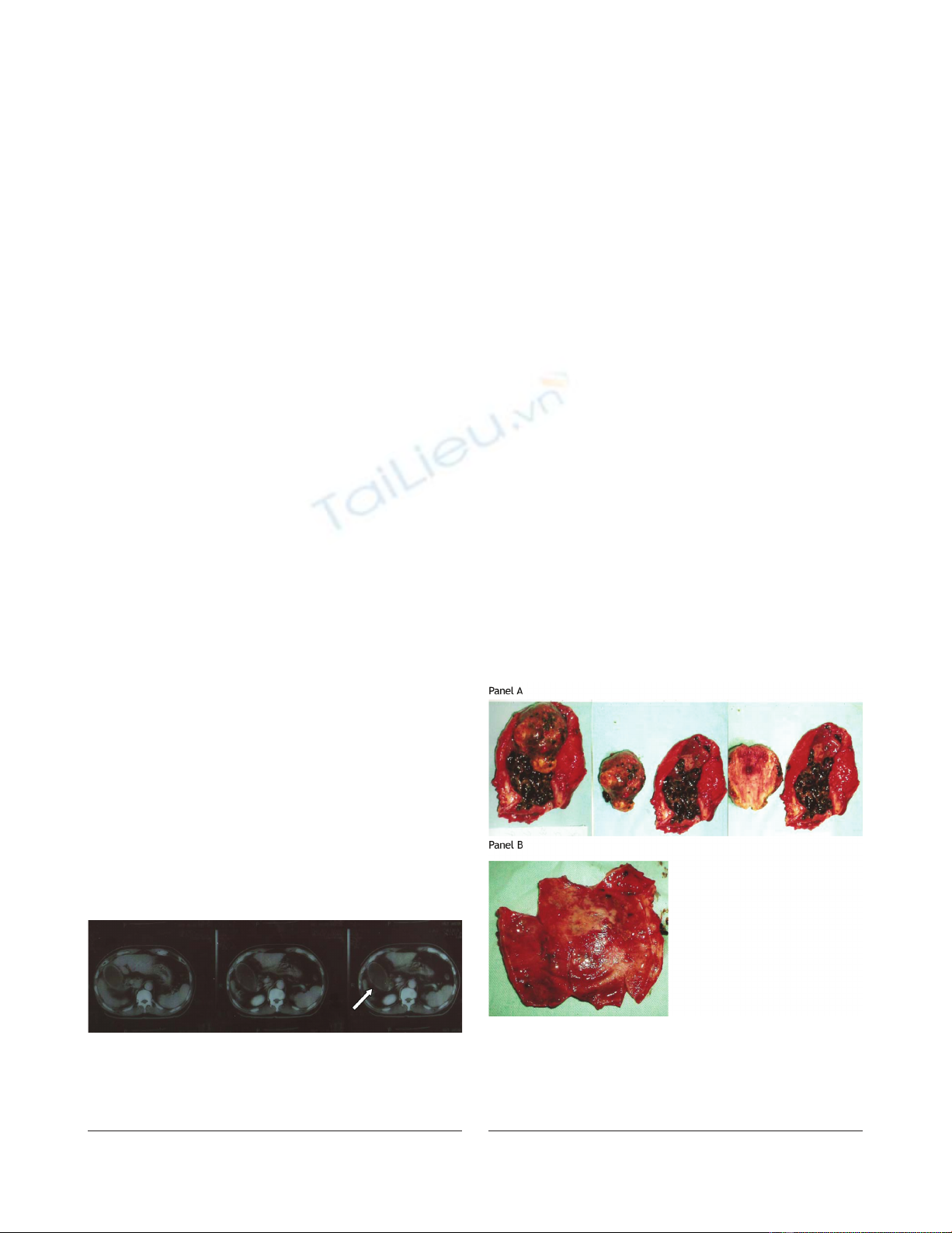
Figure 1. Computed tomography findings. Gall stones,
diffusely thickened gall bladder wall with increased contrast
enhancement, and a hypodense mass lesion (arrow) without
contrast enhancement are noted in the gall bladder lumen.
Figure 2. Operative findings. Panel A. Inflammatory gall
bladder contains multiple gall stones and a tumor measuring
6.0 ¥4.0 ¥2.0 cm. Panel B. The mucosal surface of the
gall bladder is hemorrhagic but smooth without evident
tumorous or ulcerative lesions.
Page 2 of 4
(page number not for citation purposes)
Journal of Medical Case Reports 2009, 3:7303 http://jmedicalcasereports.com/jmedicalcasereports/article/view/7303
The patient recovered from the surgery well without major
or minor complications and was discharged one week after
the surgery. He received regular follow-up in our gastro-
intestinal (GI) outpatient department and his a-FP levels
went down to 3.1 ng/mL in March 2005, and to 3.08 ng/mL
in August 2005, five and 10 months after cholecystectomy,
respectively. He died in July 2006 in another hospital due
to upper gastrointestinal bleeding from a hemorrhagic
duodenal ulcer complicated by hepatorenal syndrome.
Discussion
a-FP is a serum glycoprotein elevating in pregnancy and
pathologic tumor growth such as HCC and germ cell
tumors. It is used to evaluate treatment and to detect
recurrence of these tumors. Sometimes, gall bladder tumors
also produce a-FP because the gall bladder and liver have
identical embryologic origin. Recurrence or metastasis of
these tumors can be detected by a relapsing a-FP level [1].
Gall bladder tumors, either primary or metastasis, are rare
and often diagnosed at a late stage because of asympto-
matic properties when small and without biliary tract
obstruction. Primary a-FP producing gall bladder tumors
consist of several cell types, including undifferentiated
carcinoma, papillary clear cell carcinoma and hepatoid
carcinoma. It is possible that these a-FP producing gall
bladder tumors may have cell types within the two
extremes of the spectrum, undifferentiated carcinoma
and well differentiated hepatoid carcinoma [2]. We regard
our patient to be a unique rare case of a-FP producing
well-differentiated hepatoid carcinoma presenting as an
intraluminal growing tumor mass in the gall bladder sac
without wall invasion. No identical scenario has been
reported in the literature.
Undifferentiated gall gladder carcinoma has been reported
in an autopsy specimen by Ng and Ng [3]. Brown and
Roberts described a papillary type gall bladder adenocar-
cinoma with a-FP producing properties [4]. St Laurent
et al. also reported two a-FP producing gall bladder
tumors with direct invasion to liver showing cell types of
primary undifferentiated carcinoma and a poorly differ-
entiated tumor with a wide range of polymorphism
containing hepatoid differentiation, respectively [4]. As
for metastatic lesions, gall bladder carcinomas, although
rare, may metastasize to the liver by direct invasion [2] and
with distant metastasis to the lung [1]. HCC metastasis to
the gall bladder is much rarer. Terasaki et al. reported an
autopsy result showing HCC with gall bladder metastasis
presenting with massive intraluminal growth [5]. Chiba
et al. reported another autopsy case of HCC with gall
bladder metastasis also presenting with intraluminal
tumor growth [6]. Both of these two autopsied HCC
metastases to the gall bladder were continuous with the
gall bladder wall and tumor emboli in dilated vessel
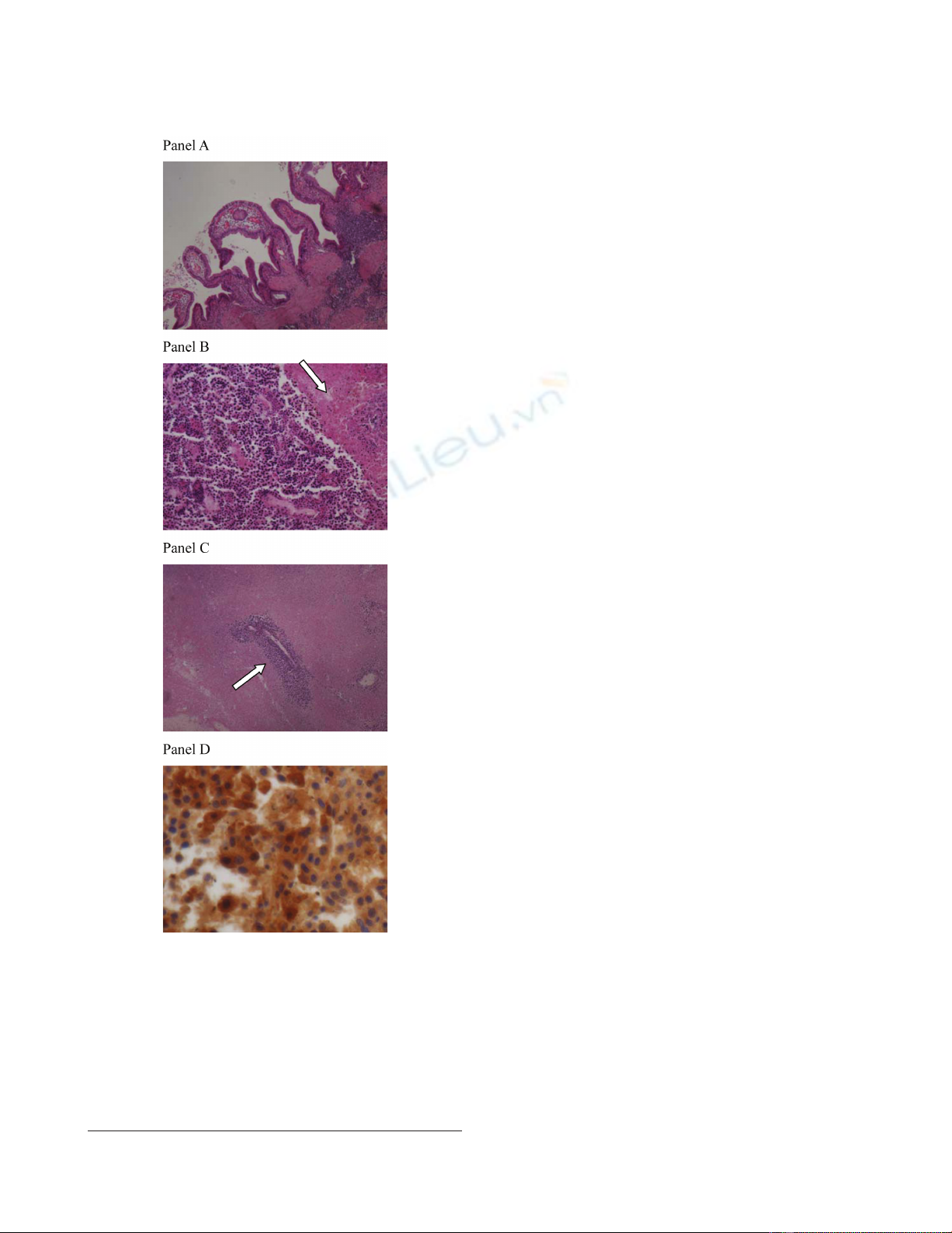
Figure 3. Pathologic examination. Panel A. Gall bladder:
Neutrophil and lymphocyte infiltration indicate acute and
chronic inflammation compatible with cholecystitis. Panel B.
Hepatoid carcinoma with the histologic feature of uniform
cells with eosinophilic cytoplasm arranged in a tile-like array
or microtrabecular pattern. Infarction necrosis is seen in the
right upper field (arrow). Panel C. Viable tumor cells are
mostly found surrounding the blood vessels (arrow).
Panel D. Immunostaining for alpha-fetoprotein demonstrates
varied staining intensity in the cytoplasm of the tumor cells.
Page 3 of 4
(page number not for citation purposes)
Journal of Medical Case Reports 2009, 3:7303 http://jmedicalcasereports.com/jmedicalcasereports/article/view/7303
lumens, and the latter character led to the postulation of
vessel route metastasis. A lesser possibility of the mechan-
ism of direct invasion was discussed in the literature
because it is quite rare for HCC to destroy the muscle layer
and collagen fibers of the gall bladder wall [6].
In our patient, an intraluminal growing gall bladder tumor
with intact gall bladder wall was found and microscopic
examination revealed uniformly well differentiated hepa-
toid carcinoma without tumor emboli in vessels. The
patient recovered from the operation without major or
minor complications and a normal a-FP level was noted
10 months after the surgery, and 20 months after cessation
of palliative oral chemotherapy. We believe that primary
a-FP producing gall bladder tumors have undifferentiated
cell type or polymorphic pattern, and that the a-FP
production may be the result of dedifferentiation. Since
our case appeared to be a uniformly well differentiated
hepatoid carcinoma after treatment of HCC, it is most
likely a metastatic lesion. Arakawa et al. reported ectopic
liver tissue with hepatocarcinogenesis [7] which is less
likely in our patient since there were no normal
hepatocytes present in the gall bladder tumor.
Conclusion
In summary, this unusual intraluminal growing tumor
proved to be a well-differentiated hepatoid carcinoma and
is most likely a metastatic lesion from previous HCC. This
case reminds clinicians that, in looking for likely HCC
recurrence, when no detectable hepatic lesion can account
for elevated a-FP levels, the gall bladder should be
included in the search for the site of metastasis.
Abbreviations
Alb, albumin; BP, blood pressure; BT, body temperature;
CT, computed tomography; ER, emergency room; HCC,
hepatocellular carcinoma; HBV, hepatitis B virus; PR,
pulse rate; RR, respiratory rate; RUQ, right upper quad-
rant; sGOT/sGPT, serum glutamic-oxaloacetic transami-
nase/serum glutamic-pyruvic transaminase; TACE,
transcatheter arterial chemoembolization; T/D, total and
direct; a-FP, alpha-fetoprotein.
Consent
Written informed consent was obtained from the patient’s
family for publication of this case report and any
accompanying images. A copy of the written consent is
available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Authors’contributions
CY was the major contributor in writing the manuscript.
CR performed the operation (open cholecystectomy) and
initiated the idea for this case report. CH performed the
histologic examination as well as the special staining
(a-FP stain) of the specimen. HT treated and followed-up
this patient. SM reviewed related articles and provided
information on the nature and course of HCC and its
setting in Taiwan. CY interpreted the image study (CT
scan) and provided radiologic information about this case.
All authors read and approved the final manuscript.
Acknowledgements
We would like to express our special gratitude to Dr Jau-
Min Lian MD/PhD, Gastroenterology of Chang Gung
Memorial Hospital, for kindly offering us the patient’s
detailed clinical history from his hospital and providing
expert professional comments on this case.
References
1. Cocquyt V, Pipeleers-Marichal M, Delvaux G, Van Belle S: Increasing
serum levels of alpha-fetoprotein in a patient with relapsing
gall bladder carcinoma. Am J Clin Oncol 1996, 19:465-468.
2. St Laurent M, Esterl RM Jr, Halff GA, Speeg KV: Gallbladder
carcinoma producing alpha-fetoprotein. J Clin Gastroenterol
1999, 28:155-158.
3. Ng WK, Ng WF: Elevated serum a-fetoprotein in a patient
with undifferentiated carcinoma of the gall bladder. J Clin
Pathol 1995, 48:1061-1063.
4. Brown JA, Roberts CS: Elevated serum alpha-fetoprotein levels
in primary gallbladder carcinoma without hepatic involve-
ment. Cancer 1992, 70:1838-1840.
5. Terasaki S, Nakanuma Y, Terada T, Unoura M: Metastasis of
hepatocellular carcinoma to the gall bladder presenting
massive intraluminal growth: report of an autopsy case.
J Clin Gastroenterol 1990, 12:714.
6. Chiba M, Saito A, Hayashi N: Hepatocellular carcinoma invades
the gall bladder via vessels. J Hepatol 2002, 37:411.
7. Arakawa M, Kimura Y, Sakata K, Kubo Y, Fukushima T, Okuda K:
Propensity of ectopic liver to hepatocarcinogenesis: case
reports and a review of the literature. Hepatology 1999,
29:57-61.
Page 4 of 4
(page number not for citation purposes)
Journal of Medical Case Reports 2009, 3:7303 http://jmedicalcasereports.com/jmedicalcasereports/article/view/7303
Do you have a case to share?
Submit your case report today
•Rapid peer review
•Fast publication
•PubMed indexing
•Inclusion in Cases Database
Any patient, any case, can teach us
something
www.casesnetwork.com


![Báo cáo seminar chuyên ngành Công nghệ hóa học và thực phẩm [Mới nhất]](https://cdn.tailieu.vn/images/document/thumbnail/2025/20250711/hienkelvinzoi@gmail.com/135x160/47051752458701.jpg)























%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)