Open Access
Available online http://ccforum.com/content/9/3/R172
R172
Vol 9 No 3
Research
Erythropoietin response in critically ill mechanically ventilated
patients: a prospective observational study
Alan J DeAngelo1, David G Bell2, Michael W Quinn1, Deborah Ebert Long3 and Daniel R Ouellette4
1Physician, Pulmonary and Critical Care Service, Dwight David Eisenhower Army Medical Center, Fort Gordon, Georgia, USA
2Fellow, Pulmonary and Critical Care Service, Brooke Army Medical Center, Fort Sam Houston, Texas, USA
3Physician, Pulmonary and Critical Care Service, David Grant Air Force Medical Center, Travis Air Force Base, California, USA
4Pulmonary and Critical Care Service, Brooke Army Medical Center, Fort Sam Houston, and Assistant Program Director PCCM fellowship, Brooke
Army Medical Center, Fort Sam Houston, Texas, USA
Corresponding author: Alan J DeAngelo, adeangelo@pol.net
Received: 18 Nov 2004 Revisions requested: 8 Dec 2004 Revisions received: 19 Dec 2004 Accepted: 27 Jan 2005 Published: 25 Feb 2005
Critical Care 2005, 9:R172-R176 (DOI 10.1186/cc3480)
This article is online at: http://ccforum.com/content/9/3/R172
© 2005 DeAngelo et al.; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/
2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction Anemia is a common problem in critically ill
patients. The etiology of anemia of critical illness is often
determined to be multifactorial in the clinical setting, but the
pathophysiology remains to be elucidated. Erythropoietin (EPO)
is an endogenous glycoprotein hormone that serves as the
primary stimulus for erythropoiesis. Recent evidence has
demonstrated a blunted EPO response as a factor contributing
to anemia of critical illness in specific subsets of patients.
Critically ill patients requiring mechanical ventilation who exhibit
anemia have not been the subject of previous studies. Our goal
was to evaluate the erythropoietic response to anemia in the
critically ill mechanically ventilated patient.
Methods A prospective observational study was undertaken in
the medical intensive care unit of a tertiary care, military hospital.
Twenty patients admitted to the medical intensive care unit
requiring mechanical ventilation for at least 72 hours were
enrolled as study patients. EPO levels and complete blood
count were measured 72 hours after admission and initiation of
mechanical ventilation. Admission clinical and demographic
data were recorded, and patients were followed for the duration
of mechanical ventilation. Twenty patients diagnosed with iron
deficiency anemia in the outpatient setting were enrolled as a
control population. Control patients had baseline complete
blood count and iron panel recorded by primary care physicians.
EPO levels were measured at the time of enrollment in
conjunction with complete blood count.
Results The mean EPO level for the control population was
60.9 mU/ml. The mean EPO level in the mechanically ventilated
patient group was 28.7 mU/ml, which was significantly less than
in the control group (P = 0.035). The mean hemoglobin value
was not significantly different between groups (10.6 g/dl in
mechanically ventilated patients versus 10.2 g/dl in control
patients; P > 0.05).
Conclusion Mechanically ventilated patients demonstrate a
blunted EPO response to anemia. Further study of therapies
directed at treating anemia of critical illness and evaluating its
potential impact on mechanical ventilation outcomes and
mortality is warranted.
Introduction
Critically ill patients frequently develop anemia during their
intensive care unit (ICU) course. Corwin and coworkers [1]
reported that 95% of patients demonstrated abnormal hemo-
globin concentration by the third ICU day. Anemia in the ICU
patient has been reported to resemble anemia of chronic dis-
ease in its metabolic pattern [2]. The etiology of anemia of crit-
ical illness is multifactorial; it often results from a combination
of primary losses, abnormal coagulation, nutritional deficien-
cies, depressed bone marrow production, and phlebotomy.
Recent evidence has demonstrated a blunted erythropoietin
(EPO) response to be a factor contributing to anemia of critical
illness in specific subsets of patients, including those with
sepsis, multiple trauma, and pediatric critical illness [3-5]. The
EPO = erythropoietin; FiO2 = fractional inspired oxygen; ICU = intensive care unit; PaO2 = arterial oxygen tension; rHuEPO = recombinant human
erythropoietin.

Critical Care Vol 9 No 3 DeAngelo et al.
R173
EPO response in adult patients requiring mechanical ventila-
tion for respiratory failure has not been studied as a primary
end-point.
EPO is an endogenous glycoprotein hormone that serves as
the primary stimulus for erythropoiesis. The kidney is the pri-
mary site of EPO production, but the liver also produces the
hormone. EPO acts in the bone marrow, where it promotes ter-
minal differentiation of progenitor cells into erythrocytes [6].
Diminished arterial oxygen content associated with anemia or
hypoxia is the major stimulus for EPO production and usually
produces an exponential increase [7-9].
Anemia of critical illness and blood management strategies in
the ICU continue to be areas of active research. Two recent tri-
als [10,11] demonstrated a reduction in the number of trans-
fusions in critically ill patients treated with recombinant human
EPO (rHuEPO). Mortality and adverse clinical events were not
statistically different between groups in either study. Hebert
and coworkers [12] investigated the effects of a restrictive
(threshold 7 g/dl, goal 7–9 g/dl) versus a liberal (threshold 10
g/dl, goal 10–12 g/dl) transfusion strategy in critically ill
patients. The authors noted a similar overall 30-day mortality
rate between groups but a significantly lower 30-day mortality
rate for less acutely ill patients in the restrictive group (Acute
Physiology and Chronic Health Evaluation II score <20 and
age <55 years). The mortality rate was higher in patients with
significant cardiac disease treated with the liberal strategy, but
the results did not achieve statistical significance (P = 0.69).
Mechanical ventilation is a common treatment in ICU patients
with respiratory failure. A major goal of ICU care is to reduce
the number of ventilator days. Numerous clinical factors have
an impact on the duration of mechanical ventilation. Improving
oxygen delivery to tissues is a recognized goal of ICU care, but
its specific impact on outcomes in mechanically ventilated
patients is not known. Anemia can lead to a reduction in oxy-
gen delivery. The potential impact of anemia on mechanical
ventilation outcomes continues to be evaluated, but there is
evidence to suggest a negative impact. Nevins and Epstein
[13] found that a low admission hematocrit was significantly
associated with death in patients with chronic obstructive pul-
monary disease receiving mechanical ventilation. Khamiees
and coworkers [14] reported that mechanically ventilated
patients with low hemoglobin levels are more likely to be
unsuccessfully extubated than are patients with higher hemo-
globin levels. Ouellette and colleagues [15] reported that a
low hemoglobin level during a period of mechanical ventilation
was the most significant risk factor for failure to wean from
mechanical ventilation.
We hypothesized that critically ill patients requiring mechani-
cal ventilation have an inadequate EPO response to anemia,
which contributes to the development and persistence of ane-
mia of critical illness.
Materials and methods
The study was approved by the Institutional Review Board at
Brooke Army Medical Center and was performed in accord-
ance with the ethical standards laid down in the 1964 Decla-
ration of Helsinki. All participants (or surrogates) were
counseled and informed consent was obtained before entry
into the study.
Study patients
Adult patients (>18 years) admitted to the medical ICU of
Brooke Army Medical Center with acute respiratory failure
requiring mechanical ventilation for 72 hours and with a hemo-
globin level below 13 g/dl were screened for eligibility.
Patients with a pre-existing indication for the use of rHuEPO,
including anemia associated with end-stage renal disease,
cancer, or cancer therapy, and those with HIV infection treated
with zidovudine were excluded. Patients with acute or chronic
bleeding of any etiology and those who received rHuEPO
either before admission or during the ICU course were also
excluded. Transfusion thresholds and goals and mechanical
ventilation management was at the discretion of the attending
physician. Transfusion guidelines outlined by Hebert and cow-
orkers [12] and the American College of Chest Physicians
weaning guidelines [16] were provided as a reference, and
adherence to these practices was encouraged. In total, 20
study patients were enrolled from January 2003 to December
2003.
Demographic and clinical data including Acute Physiology and
Chronic Health Evaluation II scores were recorded at study
entry. Admission complete blood count and basic metabolic
panel were reviewed. After study enrollment, hemoglobin and
EPO levels at day 3 were recorded for statistical analysis, and
the arterial oxygen tension (PaO2)/fractional inspired oxygen
(FiO2) ratio at day 3 was calculated. Patients were followed for
the duration of mechanical ventilation.
Control group
The control group consisted of 20 ambulatory patients with a
new diagnosis of iron deficiency anemia (hemoglobin <13 g/
dl, ferritin <100 ng/ml, iron <46 µg/dl) screened from a pri-
mary care clinic. All patients were free of acute illness, had nor-
mal renal function, and had not received rHuEPO during the
preceding 30 days. Demographic data and hemoglobin and
EPO levels were recorded for statistical analysis.
Erythropoietin assay
Serum EPO levels were measured using a commercial two-
site chemiluminescence immunoassay (Nichols Advantage
Erythropoietin Assay; Nichols Institute Diagnostics, San Clem-
ente, CA, USA) referenced to the World Health Organization
recombinant DNA-derived human EPO 1st International
Standard (WHO 87/684). Expected values were determined
from data on 119 healthy adults (age range 18–69 years). The
results ranged from <5.0 to 25.1 mU/ml. The 95% confidence

Available online http://ccforum.com/content/9/3/R172
R174
interval was 5.0–24.6 mU/ml. Reproducibility was determined
according to the National Committee for Clinical Laboratory
Standards EP5-T2 tentative guidance document [17]. The
limit of detection is estimated to be 1.2 mU/ml. The limit of
detection was determined from 20 replicate determinations of
the zero standard and is defined as the value two standard
deviations above the mean of the 20 replicates. The functional
sensitivity is estimated at 5.0 mU/ml. The functional sensitivity
is based on the lowest concentration of EPO in serum where
the interassay precision does not exceed a 20% coefficient of
variation.
Statistical analysis
Independent samples t-test was used to evaluate differences
in age, hemoglobin, and EPO by group. Paired t-test was used
to compare observed versus expected EPO levels by group. A
linear regression on EPO as a function of hemoglobin level by
group was performed. The results were expressed as mean ±
standard deviation. P < 0.05 was considered statistically
significant.
Results
Twenty (5 male, 15 female; mean age 70 years, range 49–88
years) critically ill patients requiring mechanical ventilation for
acute respiratory failure were enrolled in the study. Table 1
summarizes the study patients' characteristics. Of the 20
study patients, 18 had a PaO2/FiO2 ratio on day 3 of less than
300. Hemoglobin and EPO values were compared with those
of 20 (5 male, 15 female; mean age 60 years, range 24–84
years) control patients with iron deficiency anemia.
There was no significant difference in hemoglobin level
between the groups (mean hemoglobin 10.6 ± 1.5 g/dl in the
study group versus 10.2 ± 1.0 g/dl in the control group; inde-
pendent samples t-test, P = 0.381). Because there was no dif-
ference between groups with respect to hemoglobin, we
compared the groups with respect to EPO level. A significantly
lower EPO level was recorded in the mechanically ventilated
patient group (mean EPO level 28.7 ± 30.4 mU/ml in the study
group versus 60.9 ± 58.3 mU/ml in the control group; inde-
pendent samples t-test, P = 0.035).
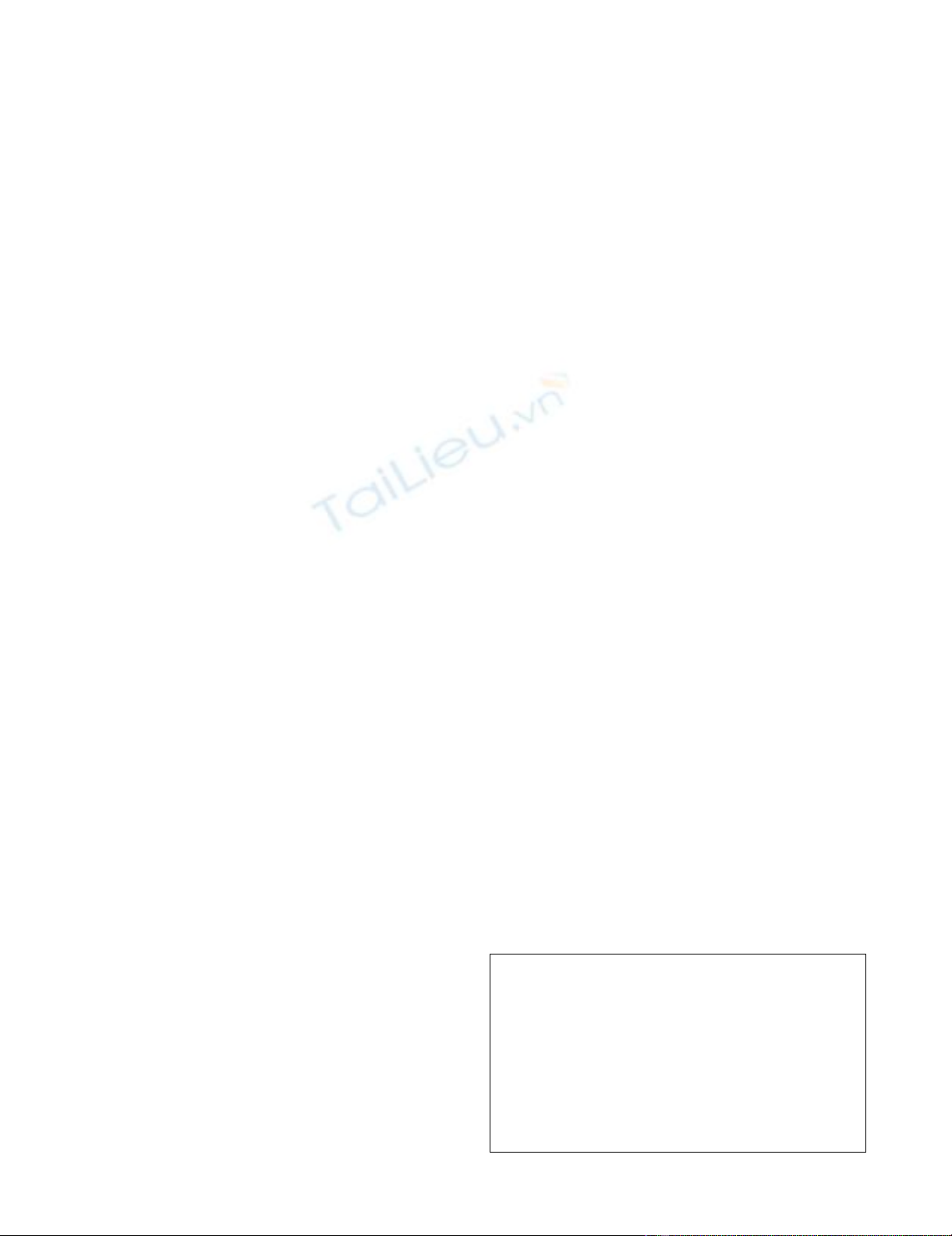
A linear regression of EPO as a function of hemoglobin was
performed to confirm the difference between expected and
observed EPO levels between groups (Fig. 1). There was no
significant difference between the observed and expected lev-
els of EPO in the control group (P = 1.000), but there was a
statistically significant difference in the study group (P =
0.006).
Discussion
Anemia in the ICU is a common problem, with a multifactorial
etiology. We evaluated the relationship of the endogenous
EPO response to anemia in the setting of mechanical ventila-
tion and demonstrated a significantly diminished response in
this population. Ambulatory iron deficient anemic patients
were chosen as control patients in order to match the
expected degree of anemia in ICU patients. Additionally, this
population demonstrated an elevated EPO response to ane-
mia in a previous study [3]. The EPO response in critical illness
has been evaluated in specific subsets of patients but not in
mechanically ventilated adult patients in a controlled design.
Rogiers and coworkers [3] compared a mixed population of
critically ill patients with iron deficient control patients to deter-
mine whether a relationship between EPO response and
degree of anemia existed. The study group consisted of 22
septic patients (subgroups with and without renal failure) and
14 nonseptic patients (subgroups with and without renal fail-
ure). Patients considered hypoxemic (PaO2 <75 mmHg) were
excluded from the analysis. The control group comprised 18
Table 1
Clinical profile of enrolled mechanically ventilated patients
Parameter Value
n20
Age (years; mean [range]) 70 (49–88)
Male/female 5/15
PaO2/FiO2 ratio (mean [range]) 220 (118–385)
APACHE II score (mean [range]) 19.8 (8–36)
Ventilator days (mean [range]) 12.3 (3–56)
Diagnosis (n)
Pneumonia 8
COPD 5
Pulmonary embolus 1
CHF/cardiac ischemia 4
Acute renal failure 2
APACHE, Acute Physiology and Chronic Health Evaluation; CHF,
congestive heart failure; COPD, chronic obstructive pulmonary
disease; FiO2, fractional inspired oxygen; PaO2, arterial oxygen
tension.
Figure 1
Linear regression: erythropoietin as a function of hemoglobinLinear regression: erythropoietin as a function of hemoglobin. The line
represents the best fit to the values in the control group.
Critical Care Vol 9 No 3 DeAngelo et al.
R175
ambulatory iron deficient patients without acute illness. Hema-
tocrit values were similar between study and control patients.
A significant inverse correlation between hematocrit and EPO
was found in the control patients and in the nonseptic patients
without renal failure. The correlation of EPO with hematocrit
was lost in the septic patients and in the nonseptic patients
with acute renal failure. The authors concluded that the EPO
response to anemia is severely blunted in critically ill patients.
Krafte-Jacobs and coworkers [5] demonstrated a blunted
EPO response in critically ill pediatric patients with acute ane-
mia and acute hypoxia. Enrolled patients included 21 with
acute anemia, 18 with acute hypoxemia (normal hemoglobin),
10 critically ill without anemia or hypoxemia, and 21 outpa-
tients with chronic anemia but no acute illness. Hemoglobin
levels were equivalent in the acutely anemic and chronically
anemic patients. The EPO levels were similar in the acutely
anemic, acutely hypoxemic, and critically ill control patients,
but significantly less than the EPO levels in the chronically
anemic patients. The authors concluded that the EPO
response to known physiologic stimuli is blunted in critically ill
children.
Hobisch-Hagen and coworkers [4] found no correlation
between EPO and hemoglobin concentrations in 23 adult
patients suffering from severe trauma. That observational
study did not include a control group for comparison. Trauma
patients exhibited anemia (mean hemoglobin 10.0 g/dl) on
admission without significant increase during the period of
observation. The mean EPO level was 49.8 U/l on day 1 with-
out significant increase throughout the study period (to day 9).
The authors concluded that patients with multiple trauma
exhibit an inadequate EPO response to low hemoglobin
concentrations.
In theory, the treatment of anemia in mechanically ventilated
patients with respiratory failure should improve oxygen delivery
to the tissues. The interplay of the other principal determinants
of oxygen delivery (cardiac output and arterial oxygen satura-
tion) and the overall impact on outcome continues to be eval-
uated. Hebert and coworkers [18] reported the impact of a
liberal (threshold hemoglobin 10.0 g/dl, goal 10–12 g/dl)
compared with a restrictive (threshold hemoglobin 7.0 g/dl,
goal 7–9 g/dl) transfusion strategy in 713 mechanically venti-
lated patients, representing a subgroup of a larger study [12].
That study found no difference in the duration of mechanical
ventilation between groups.
An adverse impact of anemia on outcome in mechanically ven-
tilated patients has been reported. Khamiees and coworkers
[14] conducted a prospective study of predictors of extuba-
tion outcome in 91 patients recovering from acute respiratory
failure and who successfully completed a spontaneous breath-
ing trial. Patients with hemoglobin values under 10 g/dl were
five times as likely to have unsuccessful extubation as those
patients with hemoglobin above 10 g/dl. To investigate predic-
tors of outcome, Nevins and Epstein [13] conducted a retro-
spective cohort study of 166 patients with chronic obstructive
pulmonary disease requiring mechanical ventilation for acute
respiratory failure of diverse etiologies. Univariate analysis
demonstrated lower admission hematocrit to be one of several
factors associated with higher in-hospital mortality. Ouellette
and colleagues [15] reported that a hemoglobin level under 9
g/dl was the most significant risk factor for unsuccessful extu-
bation in a retrospective review of laboratory parameters and
their impact on mechanical ventilation outcomes.
The etiology of anemia of critical illness remains unclear, but a
blunted endogenous EPO response appears to play a role.
The mechanisms that underlie the blunted endogenous EPO
response also remain to be elucidated, although recent stud-
ies have demonstrated this response across a spectrum of
critically ill patients, suggesting that the presence of critical ill-
ness rather than any specific diagnosis is the key factor.
Patients with hypoxia – an additional stimulus for endogenous
EPO production – were excluded in the aforementioned stud-
ies of adult patients. Despite the requirement for mechanical
ventilation and the presence of hypoxemia (mean PaO2/FiO2
<300), the critically ill patients in our study also exhibited a
blunted EPO response. These results indicate that further
investigation into the etiology as well as treatment of anemia of
critical ill patients should also include hypoxic patients requir-
ing mechanical ventilation.
Limitations of our data include the small sample size and the
observational nature of the study. It was not the objective of
the present study to determine the clinical impact of a blunted
EPO response on mechanical ventilation outcomes, which
therefore cannot be addressed.
Conclusion
In summary, we demonstrated that the EPO response to ane-
mia in the critically ill mechanically ventilated patient is blunted,
similar to findings in other previously described subsets of crit-
ically ill patients. A negative impact of anemia on outcomes in
mechanically ventilated patients has been reported. Further
study of therapies directed at treating anemia of critical illness
and determining its potential impact on mechanical ventilation
outcomes and mortality is warranted.
Key messages
• Anemia in the ICU patient is a common problem with a
multifactorial etiology.
• The EPO response to anemia in the critically ill mechan-
ically ventilated patient is blunted.
• Further investigation of therapies directed at anemia of
critically ill mechanically ventilated patients are neces-
sary to determine potential morbidity and mortality bene-
fits.

Available online http://ccforum.com/content/9/3/R172
R176
Competing interests
DRO is a member of the Speaker's Bureau and Consultant,
Ortho Biotech, and is on the Speaker's Bureau, Pfizer.
Authors' contributions
AJD modified the original protocol, executed the study, ana-
lyzed data, and drafted the manuscript. DGB assisted in exe-
cuting the study, analyzing the data, and drafting the
manuscript. MWQ and DEL participated in the original design
and coordination of the study, and in writing the original proto-
col. DRO, MWQ, and DEL conceived the study. DRO assisted
in the original design and drafting of the final manuscript. All
authors read and approved the final manuscript.
Acknowledgements
Financial support provided by Ortho-Biotech Products, LP through a
Cooperative Research and Development Agreement with the Henry M
Jackson Foundation. The opinions or assertions contained herein are the
private views of the authors and are not to be construed as reflecting the
views of the Departments of the Army, Air Force or Defense. The authors
are employees of the U.S. government. This work was prepared as part
of their official duties, and as such, there is no copyright to be
transferred.
References
1. Corwin HL, Rodriguez RM, Pearl RG, Enny C, Corwin MJ, Get-
tinger A: Erythropoietin response in critically ill patients
[abstract 143]. Crit Care Med 1997:A82.
2. Corwin HL, Krantz SB: Anemia of the critically ill: 'acute' anemia
of chronic disease. Crit Care Med 2000, 28:3098-3099.
3. Rogiers P, Zhang H, Leeman M, Nagler J, Neels H, Melot C, Vin-
cent JL: Erythropoietin response is blunted in critically ill
patients. Intensive Care Med 1997, 23:159-162.
4. Hobisch-Hagen P, Wiedermann F, Mayr A, Fries D, Jelkmann W,
Fuchs D, Hasibeder W, Mutz N, Klingler A, Schobersberger W:
Blunted erythropoietic reponse to anemia in multiply trauma-
tized patients. Crit Care Med 2001, 29:743-747.
5. Krafte-Jacobs B, Levetown ML, Bray GL, Ruttimann UE, Pollack
MM: Erythropoietin response to critical illness. Crit Care Med
1994, 22:821-826.
6. Erslev AJ: Erythropoietin. N Engl J Med 1991, 324:1339-1344.
7. Jelkmann W: Erythropoietin: structure, control of production
and function. Physiol Rev 1992, 72:449-489.
8. Erslev AJ, Caro J, Miller O, Silver R: Plasma erythropoietin in
health and disease. Ann Clin Lab Sci 1980, 10:250-257.
9. Eckardt KU, Boutellier U, Kurtz A, Schopen M, Koller EA, Bauer C:
Rate of erythropoietin formation in humans in response to
hypobaric hypoxia. J Appl Physiol 1989, 66:1785-1788.
10. Corwin HL, Gettinger A, Rodriguez RM, Pearl RG, Gubler KD,
Enny C, Colton T, Corwin MJ: Efficacy of recombinant human
erythropoietin in the critically ill patient: a randomized, double-
blind, placebo-controlled trial. Crit Care Med 1999,
27:2346-2350.
11. Corwin HL, Gettinger A, Pearl RG, Fink MP, Levy MM, Shapiro MJ,
Corwin MJ, Colton T: Efficacy of recombinant human erythro-
poietin in critically ill patients: a randomized controlled trial.
JAMA 2002, 288:2827-2835.
12. Hebert PC, Wells G, Blajchman MA, Marshall J, Martin C,
Pagliarello G, Tweeddale M, Schweitzer I, Yetisir E: A multicenter,
randomized, controlled clinical trial of transfusion require-
ments in critical care. N Engl J Med 1999, 340:409-417.
13. Nevins ML, Epstein SK: Predictors of outcome for patients with
COPD requiring invasive mechanical ventilation. Chest 2001,
119:1840-1849.
14. Khamiees M, Raju P, DeGirolamo A, Amoateng-Adjepong Y, Man-
thous CA: Predictors of extubation outcome in patients who
have successfully completed a spontaneous breathing trial.
Chest 2001, 120:1262-1270.
15. Ouellette DR, Quinn MW, Emmons EE, Gallup RA: Decreased
hemoglobin associated with impaired weaning from mechan-
ical ventilation [abstract]. Am J Resp Crit Care Med 2000,
160:A560.
16. MacIntyre NR, Cook DJ, Ely EW, Epstein SK, Fink JB, Heffner JE,
Hess D, Hubmayer RD, Scheinhorn DJ: Evidence-based guide-
lines for weaning and discontinuing ventilatory support: a col-
lective task force facilitated by the American College of Chest
Physicians; the American Association for Respiratory Care;
and the American College of Critical Care Medicine. Chest
2001, 120:375S-395S.
17. National Committee for Clinical Laboratory Standards: Evaluation
of Precision Performance of Clinical Chemistry Devices: Tentative
Guideline: NCCLS document EP5-T2 2nd edition. Wayne, PA:
National Committee for Clinical Laboratory Standards; 1992.
18. Hebert PC, Blajchman MA, Cook DJ, Yetisir E, Wells G, Marshall
J, Schweitzer I: Do blood transfusions improve outcomes
related to mechanical ventilation? Chest 2001,
119:1850-1857.


























%20--%3e%3cdefs%3e%3cstyle%3e%20.st0%20{%20fill:%20%23fff;%20}%20.st1%20{%20fill:%20%237800fa;%20}%20%3c/style%3e%3c/defs%3e%3cpath%20class='st1'%20d='M117.78,12.18H43.11c2.9,3.47,4.65,7.94,4.65,12.82,0,5.6-2.3,10.66-6.01,14.29h76.02l7.22-13.56-7.22-13.56Z'/%3e%3cg%3e%3cpath%20class='st0'%20d='M53.58,26.17h-.59v-1.46h.59v-4.96h2.83c1.78,0,2.67.94,2.67,2.82v5.76c0,1.87-.89,2.81-2.67,2.81h-2.83v-4.96ZM55.36,21.37v3.34h1.1v1.46h-1.1v3.34h1.01c.61,0,.91-.37.91-1.1v-5.93c0-.74-.3-1.1-.91-1.1h-1.01Z'/%3e%3cpath%20class='st0'%20d='M65.99,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM65.28,18.04c-.25.46-.51.77-.75.94-.21.15-.47.22-.79.22-.26,0-.57-.07-.92-.22l-.38-.15c-.14-.05-.26-.07-.37-.07-.3,0-.53.18-.71.54l-.91-.68c.25-.46.51-.77.75-.94.21-.14.48-.21.79-.21.26,0,.57.07.92.21l.38.15c.14.05.26.07.37.07.3,0,.53-.18.71-.54l.91.68ZM61.91,27.52h1.73l-.87-5.76-.87,5.76Z'/%3e%3cpath%20class='st0'%20d='M74.53,26.89v1.52c0,1.91-.89,2.86-2.67,2.86s-2.67-.95-2.67-2.86v-5.93c0-1.91.89-2.86,2.67-2.86s2.67.95,2.67,2.86v1.11h-1.69v-1.22c0-.75-.31-1.12-.93-1.12s-.93.37-.93,1.12v6.15c0,.74.31,1.11.93,1.11s.93-.37.93-1.11v-1.63h1.69Z'/%3e%3cpath%20class='st0'%20d='M81.4,31.14h-1.8l-.31-2.07h-2.19l-.31,2.07h-1.64l1.82-11.39h2.62l1.82,11.39ZM75.9,19.2l1.52-1.91h1.71l1.51,1.91h-1.61l-.76-.95-.75.95h-1.61ZM77.32,27.52h1.73l-.87-5.76-.87,5.76ZM83.1,15.99l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M84.86,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM84.01,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M93.51,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM92.66,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3cpath%20class='st0'%20d='M98.8,31.14h-1.79v-11.39h1.79v4.88h2.03v-4.88h1.83v11.39h-1.83v-4.88h-2.03v4.88Z'/%3e%3cpath%20class='st0'%20d='M105.36,24.55h2.46v1.62h-2.46v3.34h3.09v1.63h-4.88v-11.39h4.88v1.63h-3.09v3.18ZM108.17,17.29l-1.76,1.91h-1.26l1.17-1.91h1.86Z'/%3e%3cpath%20class='st0'%20d='M112.2,19.75c1.78,0,2.67.94,2.67,2.82v1.48c0,1.87-.89,2.81-2.67,2.81h-.85v4.28h-1.79v-11.39h2.64ZM111.35,21.37v3.86h.85c.58,0,.87-.36.87-1.08v-1.71c0-.71-.29-1.07-.87-1.07h-.85Z'/%3e%3c/g%3e%3ccircle%20class='st1'%20cx='25'%20cy='25'%20r='20'/%3e%3cpath%20class='st0'%20d='M32.78,19.27c2.92,0,4.43,2.55,5.28,5.33l.71,2.17c.14.38-.33.75-.71.75h-5.61c.19-.33.24-.71.09-1.08l-.75-2.45c-.43-1.32-.99-2.64-1.79-3.77.75-.57,1.65-.94,2.78-.94h0ZM25,18.38c3.25,0,4.9,2.78,5.89,5.89l.76,2.45c.14.42-.33.8-.8.8h-11.69c-.42,0-.94-.38-.8-.8l.75-2.45c.99-3.11,2.64-5.89,5.89-5.89h0ZM25,11.35c1.74,0,3.11,1.37,3.11,3.11s-1.37,3.11-3.11,3.11-3.11-1.41-3.11-3.11,1.41-3.11,3.11-3.11h0ZM17.27,19.27c1.08,0,1.98.38,2.73.94-.8,1.13-1.37,2.45-1.74,3.77l-.8,2.45c-.14.38-.05.75.09,1.08h-5.56c-.42,0-.9-.38-.75-.75l.71-2.17c.9-2.78,2.41-5.33,5.33-5.33h0ZM17.27,12.91c1.51,0,2.78,1.27,2.78,2.83s-1.27,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM32.78,12.91c1.56,0,2.78,1.27,2.78,2.83s-1.23,2.83-2.78,2.83-2.83-1.27-2.83-2.83,1.27-2.83,2.83-2.83h0ZM27.07,28.56v.09c0,.57-.24,1.08-.61,1.46h0v.05c-.38.33-.9.57-1.46.57s-1.08-.24-1.46-.61h0c-.38-.38-.61-.9-.61-1.46v-.09h1.41v.09c0,.19.05.38.19.47v.05c.09.09.28.19.47.19s.38-.09.47-.19v-.05c.14-.09.24-.28.24-.47t-.05-.09h1.41ZM30.99,28.56v.09c0,1.65-.66,3.16-1.74,4.24-1.08,1.08-2.59,1.79-4.24,1.79s-3.16-.71-4.24-1.79l-.05-.05c-1.04-1.08-1.7-2.55-1.7-4.2v-.09h1.41v.09c0,1.27.47,2.4,1.27,3.25h.05c.85.85,1.98,1.37,3.25,1.37s2.4-.52,3.25-1.37c.85-.8,1.37-1.98,1.37-3.25v-.09h1.37ZM34.99,28.56v.09c0,2.78-1.13,5.28-2.92,7.07-1.79,1.79-4.29,2.92-7.07,2.92s-5.23-1.13-7.07-2.92c-1.79-1.79-2.92-4.29-2.92-7.07v-.09h1.41v.09c0,2.4.94,4.53,2.5,6.08,1.56,1.56,3.72,2.5,6.08,2.5s4.52-.94,6.08-2.5c1.56-1.56,2.5-3.68,2.5-6.08v-.09h1.41Z'/%3e%3c/svg%3e)