THAI NGUYEN UNIVERSITY
UNIVERSITY OF MEDICINE AND PHARMACY
ĐAM THI TUYET
SOME EPIDEMIOLOGICAL CHARACTERISTICS
AND INTERVENTION EFFECIENCY FOR
RESPIRATORY INFECTIONS IN CHILDREN UNDER 5 YEARS
AT CHO MOI DISTRICTS IN BAC KAN PROVINCE
Specialty: Social Hygiene and Health Organization
Code: 62.72.73.15
SUMMARY OF PhD THESIS
Thai Nguyen - Year 2010
The work was completed in:
Medico-Pharmaceutical University - Thai Nguyen University
Advisors:
1. Assoc. Prof.,PhD. Nguyen Thanh Trung
2. Prof.,PhD. Trưong Viet Dung
Opponent 1: ..........................................................................................
..........................................................................................
Opponent 2: ..........................................................................................
..........................................................................................
Opponent 3: ..........................................................................................
..........................................................................................
The thesis will be protected in Thesis Committee in National Level
held in Thai Nguyen Medico-Pharmaceutical University
At .............in .............., ................, 20...
The information from this thesis can be found at:
- National Library
- Learning Resource Center - Thai Nguyen University
- Library of Thai Nguyen Medico-Pharmaceutical University

1
INTRODUCTION
Acute respiratory infections are very common diseases with the
highest morbidity and mortality in children, especially pneumonia
among under-five children in developing countries.
In Viet Nam, every year about 32 - 40 million episodes of
children suffer from acute respiratory infections and about 22 –
24,000 children have died from pneumonia. In disadvantaged, remote
areas, pneumonia is still a cause of a leading death in children. Now,
acute respiratory infections in children accounts for approximately
39.7% in the community. In general, main causes of acute respiratory
infections are due to viruses, bacteria, pulmonary tuberculosis in
children and fungus. In addition, owing to the impact of risk factors
such as environmental pollutions, cramped housing, smoke of the
cooking, tobacco smoke, low birth weight, malnourished children,
diarrhea and climate changes. Mother’s early recognition of signs of
respiratory infections as well as how to care for children with
respiratory infections is still limited, especially mothers living in the
mountainous, remote areas.
So, well done to prevent acute respiratory infections in children
will reduce the morbidity and mortality in children, particularly
children under 5 years old and since that it will reduce funding to pay
for drugs, medical services in hospitals, reduce the overload by
children with acute respiratory infections treated in the hospital,
reducing time of mothers to leave work to care for sick children.
Therefore, we conducted the theme: “Several epidemiological
characteristics and interventional efficiency for acute respiratory
infections in children under 5 years old at Cho Moi district in
Bac Kan province”aiming at:
1. Describe several epidemiological characteristics and
interventional efficiency for acute respiratory infections in children
under 5 years old at Cho Moi district in Bac Kan province.
2. Identify several risk factors related to acute lower
respiratory infections .
3. Evaluate effectiveness of interventional measures for acute
respiratory infections in the community.
2
NEW CONTRIBUTIONS OF THE THESIS
The thesis has identified a situation of acute respiratory
infections in children under 5 years old in Cho Moi District, Bac Kan
province remaining high.
The study was carried out in mountainous areas, highlands,
disadvantaged areas, ethnic minorities. In there, people’s living
conditions remained poor, backward and less access to information,
and their awareness was slow, but if intervened by the health
education communication with appropriate methods such as oral
propaganda in ethnic minority languages combining with posters,
leaflets, video tapes, local simple terms, easily to understand would
bring results and attract the community to participate
The intervention measure has mobilized local human
resources, attracted the participation of the community, close
coordination between the commune health centers, village health
workers and people, easily to mobilize, possible to work at all time,
any where.
The iinterventional measure has a horizontal impact and depth:
Width: The health education communication for mothers with
children under 5 years old or caregivers for detection, classification,
treatment, care , acute respiratory infection control in children.
Depth: Medical care at Home: Children were followed up in
the households to detect and classify a disease and thus children were
cared for at home, then referred to the commune health center to
exam and treat if a severe disease. Educating knowledge, attitude,
practice for mothers aimed a change of mother’s behaviors in the
respiratory infection control among children.
The immune - enhancing drugs (Broncho-Vaxom) was firstly
used for acute respiratory infection control among children in the
mountainous community, highlands and ethnic minorities.
STRUCTURE OF THESIS
The thesis includes 107 pages, 45 tables, 8 figures, 2 photos, 3
diagrams and 147 references in which 76 are in Vietnamese and 71
are in English. Key parts of thesis: Introduction: 02 pages, Chapter 1.
Literature review: 18 pages, Chapter 2. Subjects and method: 19
pages, Chapter 3. Results: 37 pages, Chapter 4. Discussion : 28 pages
Conclusions and recommendations : 03 pages

3
CHAPTER 1:
LITERATURE REVIEW
1.1. Current status of acute respiratory infections
Currently, in developing countries, respiratory tract infectious
diseases are still a cause of a leading mortality and morbidity in
children under 5 years old, mainly due to pneumonia.. According to
the World Health Organization (WHO), every year, each child suffers
from acute respiratory infections from 4-9 times. Estimating globally,
each year about 2 billion episodes of children suffer from respiratory
infections, accounting for 19-20% of deaths in children under 5 years
old worldwide.
According to a research by Ruan I. (2005), estimating the
incidence of pneumonia episodes in children under 5 years on a
global scale showed that the incidence of pneumonia episodes in
developing countries was 0.29 episode per year per child. In
developed countries, this rate was 0.026 episode per year per child
and over 95% of pneumonia episodes in children in the world
occurred in developing countries
In 2003, a study on a situation and some main risk factors
related to respiratory infections in children under 5 years old at Thuy
Duong - Huong Thuy, Thua Thien Hue conducted by Nguyen Van
Thieu and Nguyen Huu Ky States showed that the prevalence of
acute respiratory infections in the community was still high (39.7%).
In 2007, the Central Tuberculosis and Lung Hospital and
Project of Acute Respiratory Infections in Children held a workshop
on “Deployment of project activity plan of acute respiratory
infections in children in key provinces in 2007 and the 2007-2010
period” and reported that the highest prevalence of acute respiratory
infections in recent years was in the mountainous provinces, followed
by Central Coast and Plains.
1.2. Causes and risk factors related to acute respiratory
infections
1.2.1. Causes of acute respiratory infections
Viruses were the most common causes resulting in acute lower
respiratory infections in children under 5 years old and was the
leading cause of hospitalization and death in children. The common
4
viruses included: respiratory syncytium virus (RSV), influenza virus,
para influenza and adenovirus and in which RSV was the most
important pathogenic agent for lower respiratory infection. In
developing countries, bacteria played an important role in resulting in
acute respiratory infections and mainly bacteria were pneumococcus
and H. influenzae.
1.2.2. Risk factors related to acute respiratory infections
Risk factors related to acute respiratory infections in children
were: Socio-natural environment, health systems, mother’s
knowledge, attitude, practice (KAP) and biological factors. But in the
mountainous area, these risk factors are little considered and this is
an issue that we need to think.
1.3. Several intervention measures against respiratory infections
done in the world and Vietnam
- The group of intervention : Impact on knowledge, attitude
and practice of mothers or caregivers
- The group impacting on child care health systems
- The group impacting on the socio-natural environment
- The group impacting on biological factors.
Chapter 2
SUBJECTS AND METHODS
2.1. Study subjects
- Children under 5 years (from 60 months old or younger).
- Mothers with children under 5 years old or caregivers.
- Leaders of the community: Leaders of the commune, head of
Health Department.
- Commune health workers, village health workers.
2.2. Study setting and duration
2.2.1. Setting: Cho Moi District, Bac Kan Province
2.2.2. Duration: The study was carried out from December 2006 to
January 2009
2.3. Methodology
2.3.1. Study Design
- Descriptive study: A study conducted by a cross-sectional
survey to describe a real situation of acute respiratory infections and

5
at the same time to analyze to determine factors associated with acute
lower respiratory infections.
- Intervention study: Before - after intervention design with a
control group
2.3.2. Sampling method
* Sample size for a descriptive study: Calculated by the
following formula:
()
2
2
.
12(.)
pq
nZ p
α
ε
=−
n = 1038 children
The minimum sample size was 1038 children for the
descriptive study . In fact, we investigated 1152 children.
* Sample size for a intervention study: Calculated by the
following formula:
()
(
)
(
)
()
112 2
2
,2
12
11ppp p
nZ
PP
−+ −
=−
αβ
Changing data into the formula, we have: the intervention
sample size for mothers: n = 554 mothers.
The intervention sample size for children : n= 455 children
Thus, to make sure of ethics in research, we would conduct the
intervention in all mothers with children under 5 years and all
children aged 5 years in 4 intervened communes.
2.3.3. Study indicators
Indicators on current status of acute respiratory infections
in under-five children in study settings before intervention: Clinical
examination
Indicators on association between mother’s knowledge,
practices and acute lower respiratory infections: Interviewing and
observing mother’s practices.
6
Indicators on risk factors related to acute lower
respiratory infections: Interviewing and observing a housing
conditions and hygiene.
Classification of related factors according to model of
logistic regression.
Intervention efficiency index in research.
Output index: Percentage of mothers with KAP changes
after intervention
Impact index:
* Longitudinal follow-up index in the community:
- Incidence density by year, episodes of acute respiratory
infections by season, morbidity rate after using Broncho -Vaxom
during intervention.
- Morbidity of acute respiratory infections after using Broncho- Vaxom
- Rate of children using antibiotics after using Broncho- Vaxom
* Evaluation index after intervention in a intervention group
and a control group: The prevelence of acute respiratory infections
after intervention (Compared with the prevalance before intervention)
Intervention efficiency index in qualitative research to
evaluate an acceptance of the community:
In-depth interviews, group discussions: Leaders of the
community, mothers, village health workers, commune health workers
to evaluate an acceptability of the community for intervention measures
2.4. Intervention contents
Arragement of the community, deployment of health education
communication, longitudinal follow-up of acute respiratory infections in
children in the community, preventive intervention by immune-
enhancing drugs, evaluation after intervention.
2.5. Data processing and analyzing
Data were entered and processed and analyzed by using
SPSS16.0 , Epidata, EPI-INFO, EXCEL.
7
Chapter 3
STUDY RESULTS
3.2. Some epidemiological characteristics of acute respiratory
infections in children under 5 years old at the study sites
- The prevalence rate of acute respiratory infections in children
before intervention was 43.9%, acute upper respiratory infections
(36.1%), acute lower respiratory infections (7.8%). The prevalence of
acute upper respiratory infections (AURI) in a group of children aged
36-60 months was highest (41.0%), higher than a group of children
aged 2 - <12 months (27.1%), with p <0.01. The prevalence of acute
lower respiratory infections (ALRI) in a group of children aged 2 -
<12 months was highest (11.0%), higher than a group of children 36-
60 months (4.7%), with p <0.01.
- The prevalence of acute lower respiratory infections in the
H’Mong ethnic minority children was highest (26.3%), followed by
the Dao ethnic minority children (9.9%), the Nung (9.6%), the Tay
(7.0% ) and the Kinh majority children was the lowest (6.7%). The
difference in the prevalence between the H’Mong children and the
Tay and the Kinh was statistically significant, with p<0.01. (Table 3.6)
3.3.2. Factors related to acute lower respiratory infections
- A type of temporary house and a desolate, damp condition of
house, indoor stoves, animal sheds near the house, indoor smoking
were factors associated with acute lower respiratory infections in
children. A group of children living in conditions of above –
mentioned poor housing hygiene had a higher risk of respiratory
infections from 2.28 times to 3.44 times, with p <0.05 (Table 3.12)
- The time of weaned children closely related to the situation of
acute lower respiratory infections. A group of children weaned early
(<12 months) had a risk of respiratory infections to be 7.82 times
higher than a weaned group of children (>18 months), with p<0.01.
Immunization status was also closely related to the situation of acute
lower respiratory infections in children. Children who were not fully
vaccinated or were fully vaccinated but an incorrect schedule had a
risk of acute lower respiratory infections to be 8.24 times higher than
the children who were fully vaccinated and according to a correct
schedule, with p <0.01 (Table 3.13).
8
- Mother’s knowledge on child care was closely related to
acute lower respiratory infections. Children of mothers with poor
knowledge had a risk of acute lower respiratory infections to be 3.69
times higher than children of mothers with a good and average
knowledge , with p <0.01 (Table 3.14)
- Mother’s child care practices were closely related to acute
lower respiratory infections in children. Children of mothers with
poor practices had a risk of acute lower respiratory infections to be
5.18 times higher than children of mothers with a very good and
average practices, with p <0.01 (Table 3.15).
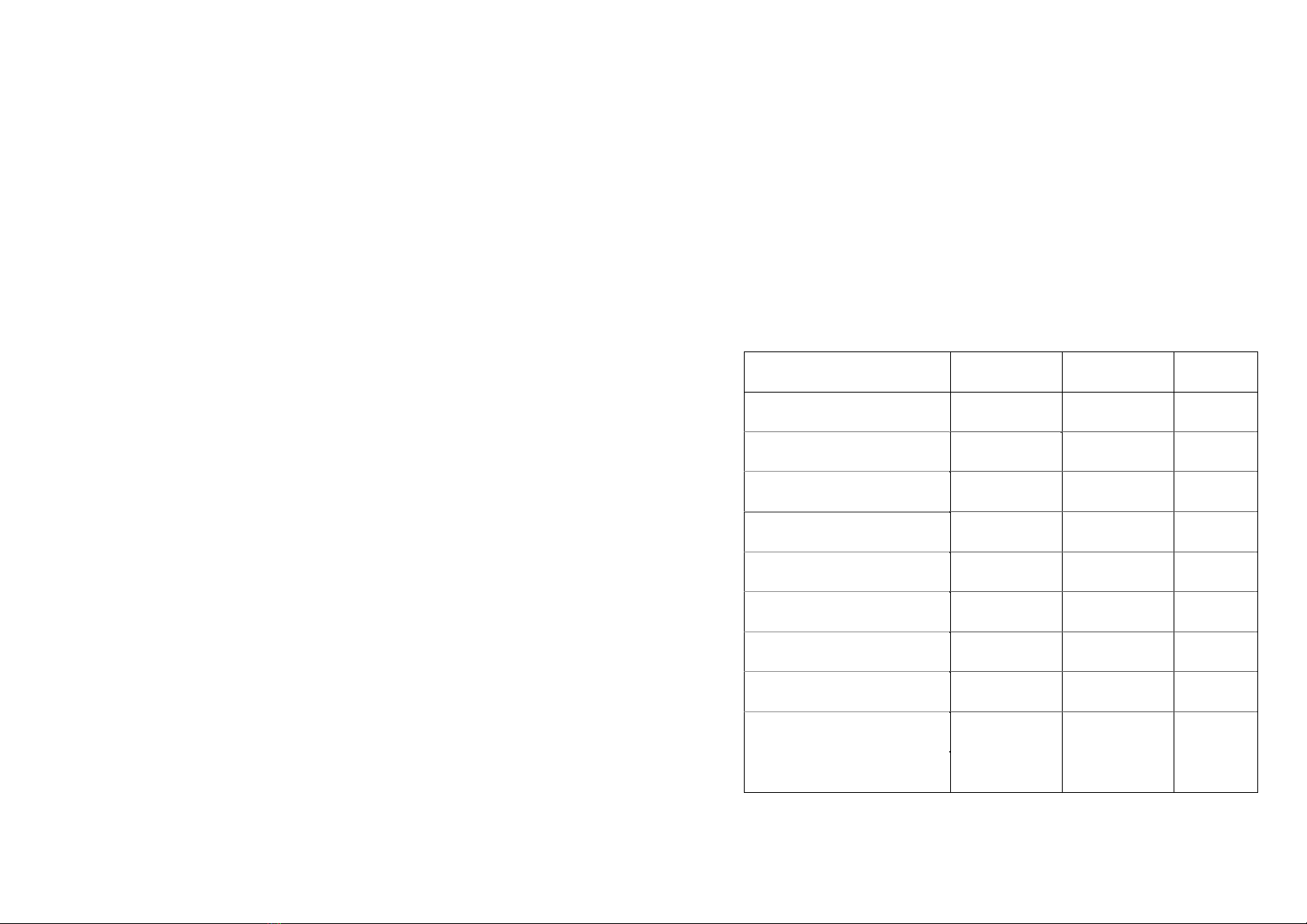
Table 3.16. Assessing related factors according to models of logistic
regression
Related factors included in
regression models
Crude OR
( 95% CI)
Adjusted OR
( 95%CI)
p
(adjusted)
Not fully vaccinated or fully
but incorrect schedule
8.24
{4.34-15.66}
10.8
{3.96-29.85} <0.01
Early weaned < 12 months
old
7.82
{3.06-17.97}
4.39
{1.82-10.56} <0.01
Poor child care practice 5.18
{2.06-13.01}
4.61
{1.82-11.67} < 0.01
Poor child care knowledge 3.69
{1.58-8.65}
3.38
{1.43-7.9} < 0.01
Type of temporary house 3.44
{1.03-11.42}
1.47
{0.83-2.62} > 0.05
Damp condition of house 3.08
{1.94-4.89}
1.85
{1.2-3.41} < 0.05
Animal sheds near the house 2.51
{1.46-4.32}
2.0
{1.14-3.52} < 0.05
Mother’s education
≤ primary school
2.46
{1.07-5.70}
1.43
{0.89-2.29} > 0.05
Smoking 2.43
{1.34-4.40}
3.29
{1.52-7.13} < 0.01
Indoor stoves 2.28
{1.46-3.57}
1.75
{1.01-3.03} < 0.05




![Luận văn Thạc sĩ: Tổng hợp và đánh giá hoạt tính chống ung thư của hợp phần lai tetrahydro-beta-carboline và imidazo[1,5-a]pyridine](https://cdn.tailieu.vn/images/document/thumbnail/2025/20250816/vijiraiya/135x160/26811755333398.jpg)