RESEARC H Open Access
Highly malignant soft tissue sarcoma of the
extremity with a delayed diagnosis
Jong Hoon Park
1*
, Chang Ho Kang
2
, Chul Hwan Kim
3
, In Jung Chae
1
, Ji Hun Park
1
Abstract
Purpose: To evaluate the characteristics of highly malignant soft tissue sarcoma of the extremity with a delayed
diagnosis.
Materials and methods: The clinical and radiological characteristics of 18 cases of highly malignant soft tissue
sarcomas of the extremity with a delayed diagnosis were determined.
Results: Ten men and eight women of mean age 44.8 years (range, 15-79 years) were included in this study. Seven
cases of synovial sarcoma, three cases each of alveolar soft part sarcoma and malignant fibrous histiocytoma, two
cases each of highly malignant leiomyosarcoma and myxofibrosarcoma, and one case of clear cell sarcoma were
enrolled. Times from tumor detection to diagnosis ranged from 1 to 3 years in most cases; three of the seven
synovial sarcoma cases took more than 10 years to diagnose. Of the seven cases of synovial sarcoma, five cases of
small, superficial located masses were simply excised without a pre-surgical biopsy. Three cases of alveolar soft part
sarcoma showed characteristic T1- and T2-weighted high signal intensities with signal voids in MR images. In
addition, one synovial sarcoma patient and one alveolar soft part sarcoma patient showed evidence of calcification
on plain radiographs. However, no general characteristic clinical findings were found to be common to the 18 cases.
Conclusions: Contrary to general expectations, some soft tissue tumors that grow slowly are painless, and those
that occur in superficial limbs may be highly malignant. Thus, even when a slow growing, painless superficial mass
is encountered in a limb, physicians should keep the possibility of highly malignant soft tissue sarcoma in mind.
Introduction
Soft tissue sarcomas that develop in the limbs and the
axial area, even those that are diagnosed early using
appropriate methods and are treated adequately, have a
5-year survival rate of between 62 and 84% [1,2]. Early
diagnosis is extremely important for the successful treat-
ment of soft tissue sarcoma. However, delayed diagnosis
of soft tissue sarcoma is common. The reasons for these
delays are variable, and include, slow-growth, no pain,
no palpation due to a deep-seated location, and doctor-
associated and socioeconomic factors. Because a sub-
stantial proportion of soft tissue sarcomas can grow for
a long time without pain, they are often misdiagnosed
due to the belief held by a large number of clinicians
and the general populations that malignant tumors are
painful, grow rapidly, and adhere strongly to adjacent
tissues, and thus, slow growing, highly malignant soft
tissue sarcomas may not be diagnosed, which is likely to
result in poor outcomes and become the basis of dis-
putes between physicians and the patient’s relatives.
Furthermore, because tumor growth rates are subjective,
no definition of a slow growing tumor exists in the lit-
erature. According to a study by Lawrence et al. [3],
approximately 60% of patients with a soft tissue sarcoma
knew they had a tumor, and these patients were diag-
nosed within 6 months of this realization. In this study,
we defined a slow-growing tumor as one that patients
had been aware of for over a year, and using this criter-
ion, we analyzed highly malignant, slowly growing soft
tissue sarcoma cases clinically and radiologically. Here,
we describe the characteristics of these tumors and pro-
vide a review of the literature.
Materials and methods
Of 31 cases with a diagnosis of highly malignant (Grade III
according to the WHO classification) soft tissue sarcoma
* Correspondence: pjh19642001@yahoo.co.kr
1
Department of Orthopedic Surgery, College of medicine, Korea University,
Anam Hospital, Seoul, Korea
Full list of author information is available at the end of the article
Park et al.World Journal of Surgical Oncology 2010, 8:84
http://www.wjso.com/content/8/1/84 WORLD JOURNAL OF
SURGICAL ONCOLOGY
© 2010 Park et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons
Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in
any medium, provided the original work is properly cited.
of the limb treated at our hospital between July 1997
and December 2008, we analyzed 18 cases in which
the delay between patient awareness of the tumor and
diagnosis exceeded 1 year. Highly malignant soft tissue
sarcoma was diagnosed based on entries in final
pathology reports. The male to female ratio of our
cohort was 10:8, and mean patient age was 44.8 years
(range 15 to 79 years). The characteristics of the 18
cases of highly malignant soft tissue sarcoma were ana-
lyzed based on tumor types determined at final diagno-
sis, times from patient recognition to diagnosis, the
anatomical locations of tumors in limbs, depths of
tumor locations in tissue (dichotomized as deep or
superficial), tumor sizes, and the characteristics of
tumors as determined by plain radiography and MRI.
Results
Seven cases of synovial sarcoma, three cases each
of alveolar soft part sarcoma and malignant fibrous
histiocytoma, two cases each of myxofibrosarcoma and
high-grade leiomyosarcoma, and one case of clear cell
sarcoma were diagnosed. Four of the seven cases of syno-
vial sarcoma, two of the three cases of alveolar soft part
sarcoma, two cases of myxofibrosarcoma, and one case
each of high-grade leiomyosarcoma and clear cell
sarcoma were transferred to our hospital after surgery or
biopsy at another hospital. For the remaining 8 cases, all
procedures from biopsy to final surgery were performed
at our hospital. Affected areas included the thigh (four
cases), the lower leg (six cases), the foot and ankle joint
(three cases), the forearm (four cases), and the popliteal
area (one case). Pulmonary metastasis was detected at
diagnosis in all alveolar soft part sarcoma cases and in
one clear cell sarcoma case. However, no distant metasta-
sis was detected in the other tumor cases. In six cases,
primary tumors were located in a deep region, and in
twelve cases, they were located superficially. All three
malignant fibrous histiocytoma cases occurred in patients
in their 70 s, whereas the alveolar soft part sarcomas
occurred in one child (>10 years old), and in one 20 and
one 30 year old. Synovial sarcomas occurred in indivi-
duals with ages at onset ranging from the second to the
sixth decade, but it occurred preferentially in adults.
Delays between tumor recognition by a patient to diagno-
sis were between 1 and 3 years in most cases. However,
in three cases of synovial sarcoma, it took more than
10 years to reach a diagnosis, and in another case of
synovial sarcoma, it took more than 5 years. In one case
of synovial sarcoma, recurrence occurred at the primary
tumor location several times over 20 years. No common
characteristic findings were evident by plain radiography,
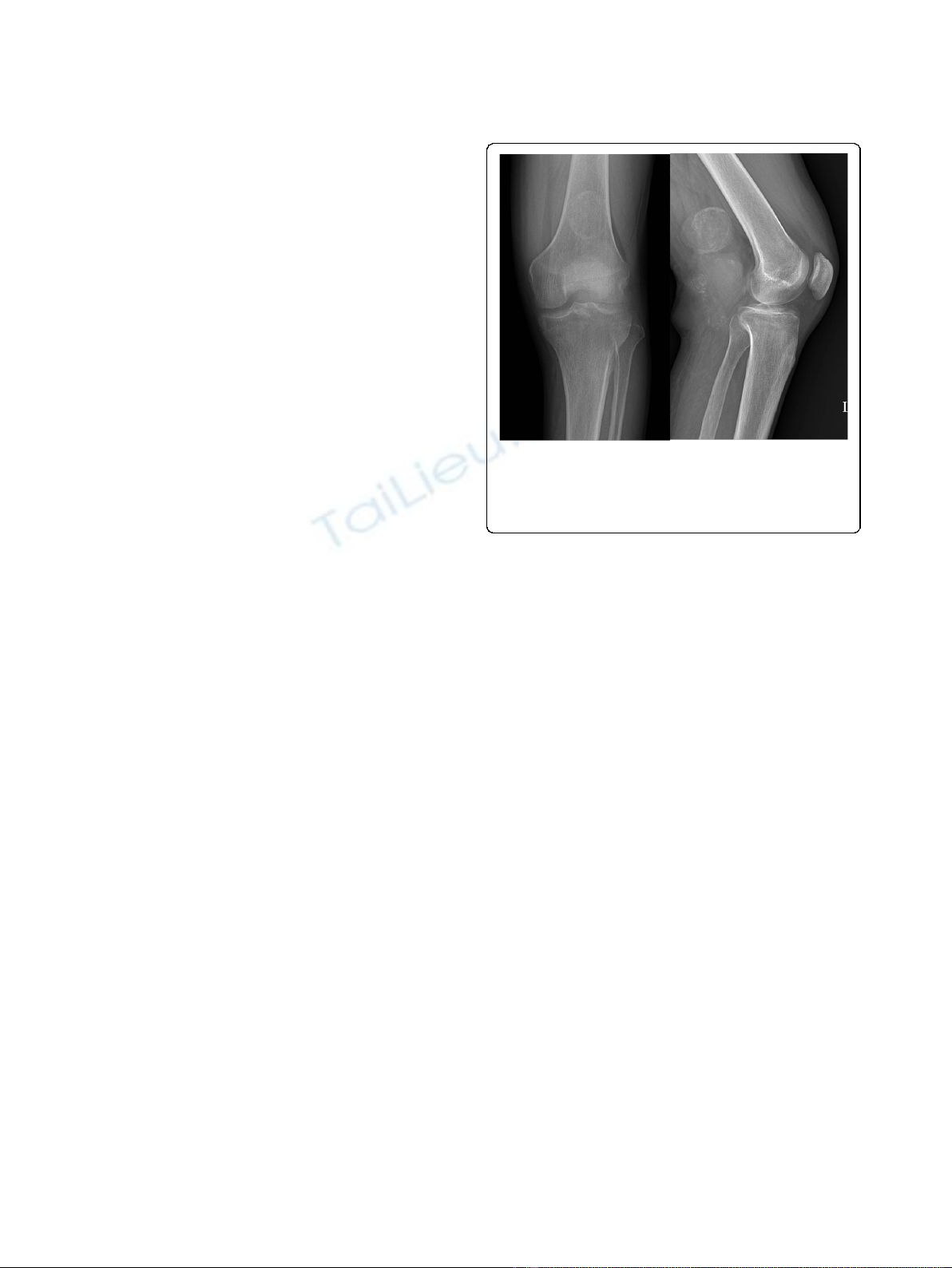
although one case of synovial sarcoma (Figure 1) and one
case of alveolar soft part sarcoma showed calcification on
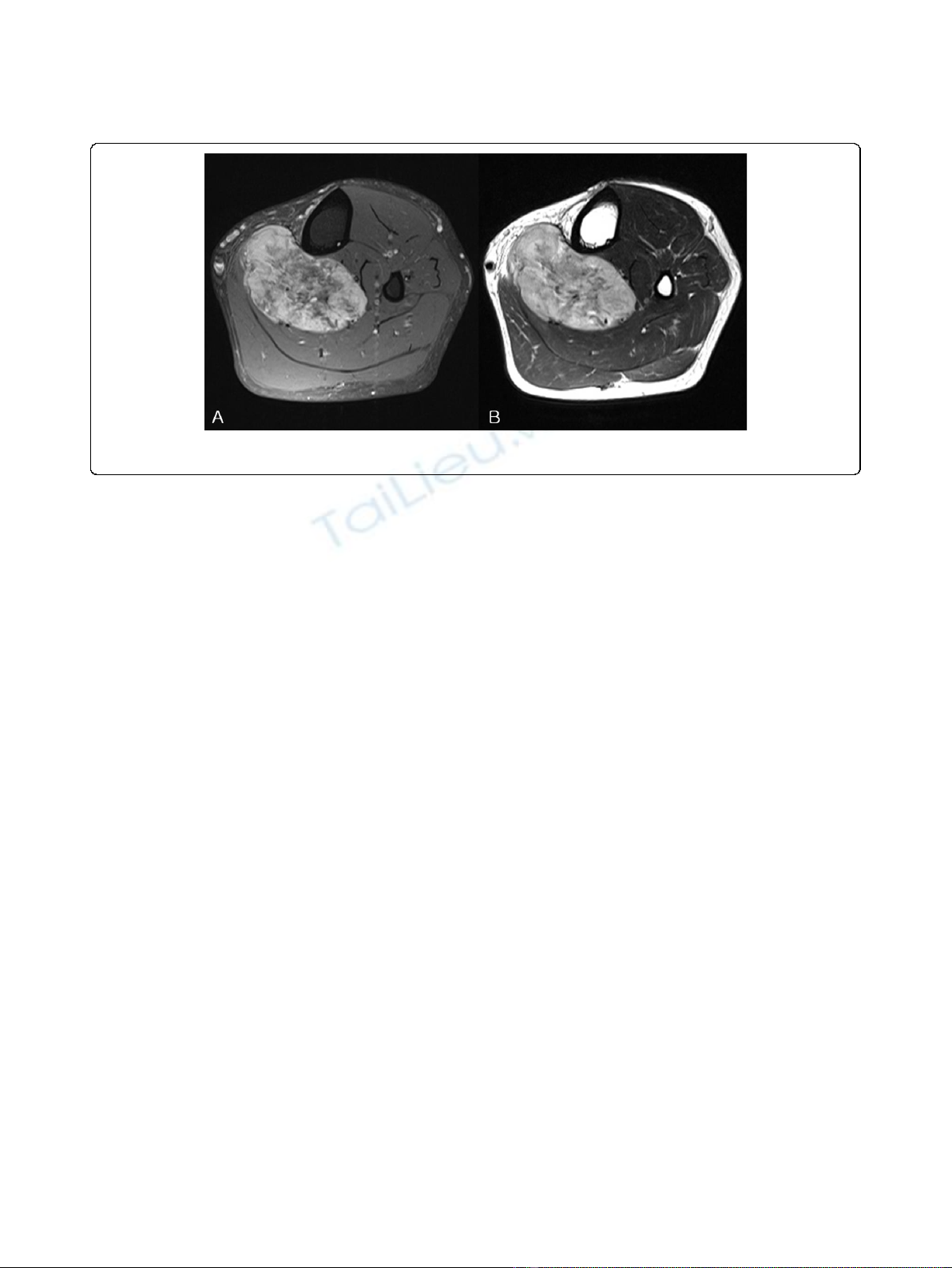
plain radiographs. In all three cases of alveolar soft part
sarcoma, the characteristic MRI finding was of high
signal intensity with signal voiding on T1 and T2 images
(Figure 2), which was attributed to the presence of abun-
dant blood vessels. However, no other tumor-specific
findings were evident. A diagnostic biopsy was only
performed in one of the seven synovial sarcoma cases.
In this case, a relatively large tumor was fixed in the
superficial layer prior to final operation. However, in the
other six cases, simple excision was performed without a
pre-surgical biopsy because tumors were small or superfi-
cially located. In contrast to synovial sarcoma cases, diag-
nostic biopsies were performed in all malignant fibrous
histiocytoma and alveolar soft part sarcoma cases due
to a relatively large tumor size or a deep location.
Discussion
Some types of soft tissue sarcoma that develop in the
limbs or axial skeleton grow slowly over several years,
or remain the same size for years or even decades, and
then suddenly start to grow. Because these tumors are
painless and movable by palpation in many cases, they
are often misdiagnosed as benign tumors, and simple
excision is performed without adequate pre-surgical eva-
luation. Importantly, if simple excision is performed
without biopsy, the tumor can recur several years later,
when all concerned will be taken aback by its aggressive
nature. Both physicians and patients have a precon-
ceived idea that malignant tumors are painful and grow
rapidly. Furthermore, soft tissue sarcomas are much
rarer than benign tumors, and thus, physicians often fail
to recommend appropriate tests or perform a compre-
hensive biopsy. In addition, patients may not even
Figure 1 A plain radiograph showing a well-defined soft tissue
mass with marginal calcification posterior to the distal femur.
There is no evidence of associated bone erosion in this patient. This
is an example of a synovial sarcoma in one of its more common
locations.
Park et al.World Journal of Surgical Oncology 2010, 8:84
http://www.wjso.com/content/8/1/84
Page 2 of 5
consider consulting a physician in some cases because
they do not consider the tumor to be serious. Tumors
thatdonotchangeorchangeonlyslowlyovertimeare
often considered benign, but tumor growth rate should
notformthebasisofadiagnosis.AccordingtoLawr-
ence et al. [3], approximately 50% of soft tissue sarcoma
patients are diagnosed at about 4 months after patient
recognition, and an additional 20% are diagnosed after
6 months. Furthermore, because the literature provides
no precise definition of ‘slowly-growing’sarcoma, we
considered a slow-growing tumor to be one known to
the patient for more than one year prior to diagnosis.
Synovial sarcoma is a representative type of slowly
growing highly malignant tumor, and it has been
reported that in synovial sarcoma cases, a substantial
proportion of patients have an average symptomatic per-
iod of 2 to 4 years, though in some rare cases, this per-
iod has been reported to be longer than 20 years [4].
Of the 18 subjects enrolled in the present study, one
case had a symptomatic period of 20 years, and four of
the seven synovial sarcoma cases had a symptomatic
period of 5-6 years (Table 1). For the reasons listed
above, the diagnosis of synovial sarcoma is frequently
delayed. In some previous studies, ~20-30% of patients
have presented with calcificationonplainradiographs
[5-7]. Similarly, in our study, calcific density was
observed by plain radiography in one case with a tumor
in the popliteal area. Sixty percent of soft tissue sarcoma
cases occur in the limbs, and the most prevalent affected
region is the distal femoral area around the knee joint
[8]. Consistent with previous studies, we found that
these tumors occurred in individuals with diverse ages
ranging from adolescents to adults. To determine the
disease stage of soft tissue sarcoma, tumor growth rate
and size, and location within tissue should be consid-
ered. Characteristics worth noting are that most highly
malignant sarcomas are located deep within limb mus-
cles, and that tumor sizes are larger than 5 cm [9].
In the present study, six of seven synovial sarcoma cases
were located in superficial areas, but these were small
tumors with a long axis of less than 5 cm in four cases.
For these reasons, six of the seven were excised without
sufficient biopsy or examination. The characteristics of
the alveolar soft portions of sarcomas are that they com-
prise only 0.5-1.0% of soft tissue sarcomas, grow slowly,
have metastasized in 20-25% of cases at diagnosis,
respond poorly to chemotherapy, and have a poor prog-
nosis [10,11]. Onset usually occurs during adolescence
or in young adults, and the only symptom is restriction
of joint movement. In our study, one of the three cases
of alveolar soft part sarcoma occurred in adolescence,
and the other two occurred in young adults. In two of
these three cases, the chief complaint was of a painless
tumor, whereas the third admitted restricted joint move-
ment with mild pain. At time of diagnosis, pulmonary
metastasis was detected in all three cases. In contrast to
other soft tissue sarcomas, alveolar soft part sarcomas
have characteristic radiologic features, that is, MRI T1-
and T2-weighted images have high signal intensities and
signal voids due to the presence of abundant blood ves-
sels [12-14]. Accordingly, these tumors can be misdiag-
nosed as hemangiomas or A-V malformations. In the
present study, one case was attributed to hemangioma
at initial examination. In alveolar soft part sarcomas,
solid tumor tissues are surrounded by vascular tissues
and blood flow wash-out is slow. In contrast, A-V
malformations are comprised of pure vascular tissue
without accompanying tissues, and blood flow wash-out
Figure 2 MRI images of an alveolar soft part sarcoma. (A) An axial T1-weighted fat-suppressed image and (B) an axial T2-weighted image.
High signal on T1FS, T2WI with multiple signal voids are apparent.
Park et al.World Journal of Surgical Oncology 2010, 8:84
http://www.wjso.com/content/8/1/84
Page 3 of 5
is rapid, which enables the differentiation of these two
conditions [14-16].
Since most soft tissue sarcomas lack defined radiologi-
cal characteristics, it is not easy to differentiate sarco-
mas, even by MRI. Nonetheless, alveolar soft part
sarcomas do have specific imaging results, and thus,
imaging tests may play a decisive diagnostic role. The
general characteristics of most sarcomas are that they
grow quickly, are located deep within tissue, and are
relatively large. As shown by the present study, the char-
acteristics of some types of soft tissue sarcomas contrast
with the traditionally held opinion that they are small
slow-growing masses with a superficial location. Fortu-
nately, non-specific soft tissue sarcomas are uncommon,
and if preconceived notions are avoided, they can be
diagnosed early. Synovial sarcoma cases occur primarily
in adults in the vicinity of the knee joint and in the
lower leg, and the tumors grow slowly and occur super-
ficially. On the other hand, alveolar soft part sarcomas
occur in adolescents and young adults, and are found
preferentially around the knee joint and have specific
MRI characteristics.
Conclusions
According to this study, some soft tissue tumors that
grow slowly are painless, and some that occur in the
superficial limbs may be highly malignant. The most
important characteristic of soft tissue sarcomas is their
non-specific nature. Thus, even when a slow growing,
painless superficial mass is encountered in the limbs,
after eliminating absolutely benign possibilities, such as,
a ganglion of the wrist or lipoma of the back, physicians
must consider the possibility of sarcoma and conduct a
careful examination.
Author details
1
Department of Orthopedic Surgery, College of medicine, Korea University,
Anam Hospital, Seoul, Korea.
2
Department of Radiology, College of medicine,
Korea University, Anam Hospital, Seoul, Korea.
3
Department of Pathology,
College of medicine, Korea University, Anam Hospital, Seoul, Korea.
Authors’contributions
JoHP drafted the manuscript, ChaHK and ChuHK participated in the design
of the study, IJC and JiHP conceived of the study, and participated in its
design and coordination. All authors read and approved the final
manuscript.
Competing interests
The authors declare that they have no competing interests.
Received: 27 June 2010 Accepted: 23 September 2010
Published: 23 September 2010
References
1. Noria A, Davis A, Kandlel R, Levesque J, O’Sullivan B, Wunder J, Bell R:
Residual disease following unplanned excision of soft tissue sarcoma of
an extremity. J Bone Joint Surg 1996, 78A:650-5.
2. Simon MA, Enneking WF: The management of soft-tissue sarcomas of the
extremities. J Bone Joint Surg 1976, 58A:317-27.
3. Lawrence W Jr, Donegan WL, Natarajan N, Mettlin C, Beart R, Winchester D:
Adult soft tissue sarcomas. A pattern of care survey of the American
College of Surgeons. Ann Surg 1987, 205(4):349-59.
4. Enzinger FA, Weiss SW: Soft tissue tumors. St. Louis, Missouri, 3 1995,
757-86.
5. Menendez LR, Brien E, Brien WW: Synovial sarcoma, A clinicopathologic
study. Orthop Rev 1992, 21:465-71.
Table 1 Clinical data of all materials
No Gender Age
(Yrs)
Duration
(Yrs)
Diagnosis Pain Location Depth Size Previous biopsy
1 M 42 6 S S No thigh deep 12 × 7 × 7 N
2 M 27 20 S S No forearm superficial 3 × 2 × 2 N
3 F 53 2 S S mild ankle superficial 1.8 × 1.2 × 0.5 N
4 F 53 10 S S mild foot superficial 5 × 5 × 6 Y
5 M 15 1 S S No ankle superficial 3 × 3 N
6 F 28 1 S S mild forearm superficial 2 × 2 N
7 M 40 10 S S Yes popliteal superficial 5 × 5 N
8 M 70 1 MFH No thigh superficial 9 × 4 Y
9 F 79 3 MFH No forearm superficial 15 × 7 Y
10 M 69 1 MFH No lower leg superficial 5 × 2 Y
11 F 16 1 Alv SS mild thigh deep 5 × 4 × 3 Y
12 M 27 3 Alv SS yes lower leg deep 7 × 4 × 11 Y
13 M 32 3 Alv SS yes lower leg deep 15 × 7 × 6 Y
14 M 72 3 HGL No thigh deep 4 × 4 × 5 Y
15 F 68 3 HGL No lower leg superficial 5 × 4 × 3 N
16 F 52 2 MFS mild lower leg superficial 14 × 9 Y
17 M 31 1 MFS mild lower leg deep 10 × 5 Y
18 F 50 1 CS No forearm superficial 2 × 3 N
M: male, F: female, S S: synovial sarcoma, MFH: malignant fibrous histiocytoma, HGL: high grade leiomyosarcoma, Alv SS: alveolar soft part sarcoma, CS: clear cell
sarcoma, MFS: myxofibrosarcoma.
Park et al.World Journal of Surgical Oncology 2010, 8:84
http://www.wjso.com/content/8/1/84
Page 4 of 5
6. Varena-Duran J, Enzinger FM: Calcifying synovial sarcoma. Cancer 1982,
50:345-52.
7. Wright PH, Sim FH, Soule EH, Taylor WF: Synovial sarcoma. J Bone Joint
Surg 1982, 64A:112-22.
8. Kransdorf MJ: Malignant soft-tissue tumors in a large referral population:
distribution of diagnoses by age, sex, and location. Am J Roentgenol
1995, 164:129-34.
9. Brennan MF: Staging of soft tissue sarcomas. Ann Surg Oncol 1999, 6:8-9.
10. Lieberman PH, Brennan MF, Kimmel M, Erlandson RA, Garin-Chesa P,
Flehinger BY: Alveolar soft part sarcoma, A clinicopathologic study of
half a century. Cancer 1989, 63:1-13.
11. Pang LM, Roebuck DJ, Griffith JF, Kumta SM, Metreweli C, Alveolar soft-part
sarcoma: A rare soft-tissue malignancy with distinctive clinical and
radiological features. Pediatr Radiol 2001, 31:196-9.
12. Iwamoto Y, Morimoto N, Chuman H, Shinohara N, Sugioka Y: The role of
MR imaging in the diagnosis of alveolar soft part sarcoma: a report of
10 cases. Skeletal Radiol 1995, 24:267-70.
13. Lorigan JG, O’keeffe FN, Evans HL, Wallace S: The radiologic manifestations
of alveolar soft-part sarcoma. Am J Roentgenol 1989, 153:335-9.
14. Suh JS, Cho J, Lee SH, Shin KH, Yang WI, Lee JH, Cho JH, Suh KJ, Lee YJ,
Ryu KN: Alveolar soft part sarcoma: MR and angiographic findings.
Skeletal Radiol 2000, 29:680-9.
15. Dobson MJ, Hartley RW, Ashieigh R, Watson Y, Hawnaur JM: MR
angiography and MR imaging of symptomatic vascular malformations.
Clin Radiol 1997, 52:595-602.
16. Lo CM, Yeung HY, Sie KF: Misdiagnosed localized arteriovenous
malformation. J Vasc Surg 1987, 6(4):419-21.
doi:10.1186/1477-7819-8-84
Cite this article as: Park et al.: Highly malignant soft tissue sarcoma of
the extremity with a delayed diagnosis. World Journal of Surgical
Oncology 2010 8:84.
Submit your next manuscript to BioMed Central
and take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at
www.biomedcentral.com/submit
Park et al.World Journal of Surgical Oncology 2010, 8:84
http://www.wjso.com/content/8/1/84
Page 5 of 5